Hoarding Disorder: Definition, Symptoms, Causes, Treatments

Hoarding disorder is characterized by persistent difficulty discarding possessions, regardless of their value. It is driven by strong urges to save items and distress when parting with them. This leads to cluttered living spaces that compromise safety and functionality, impacting daily life, relationships, and occupational functioning.
Hoarding disorder is common in about 0.98% (95% CI 0.7–1.4) of children, with a female-to-male ratio of 3:1, according to Akıncı MA et al. ‘s 2022 study, “Prevalence and Correlates of Hoarding Behavior and Hoarding Disorder in Children and Adolescents,” published in the Journal of European Child Adolescence Psychiatry.
The symptoms of hoarding disorder include excessive acquisition of unnecessary items, emotional attachment to belongings, and impaired decision-making about what to keep or discard. Affected individuals experience anxiety about others touching their possessions, social isolation, and challenges in organizing cluttered environments.
The causes of hoarding disorder are genetic predisposition, neurocognitive deficits, and life stressors. Traumatic events and attachment issues exacerbate symptoms, while cognitive-behavioural models emphasize information-processing deficits and avoidance behaviors. Socioeconomic status and age influence symptom severity, though these relationships require further study.
Cognitive behavioral therapy (CBT) is the primary evidence-based treatment of hoarding disorder. It focuses on restructuring beliefs about possessions, practicing discarding and improving organizational skills. Therapists guide individuals through home-based sessions to address clutter gradually without forcing disposal. Motivational interviewing and skills training (e.g., decision-making strategies) are integrated to enhance engagement and practical outcomes.
There were large effect sizes for hoarding symptom reduction in individual CBT (26 sessions), with 71% improved and 41% clinically significant improvement post-treatment, according to Steketee G et al. ‘s 2010 research, “Waitlist-controlled Trial of Cognitive Behavior Therapy for Hoarding Disorder,” published in the Journal of Depression Anxiety.
Medications like selective serotonin reuptake inhibitors (SSRIs) complement therapy, particularly for individuals with coexisting depression or anxiety. Treatment success depends on sustained commitment, as progress is typically gradual and requires ongoing maintenance to prevent relapse. Early intervention is critical, as untreated hoarding disorder worsens over time.
What is a Hoarding Disorder?
Hoarding disorder (HD) is a mental health condition characterized by persistent difficulty discarding or parting with possessions, regardless of their actual value. This leads to cluttered living spaces that compromise safety and functionality. Key diagnostic criteria include a perceived need to save items, distress when discarding them, and clinically significant impairment in daily life. The disorder is recognized in both the DSM-5 and ICD-11, with symptoms accompanied by excessive acquisition behaviors and emotional attachment to possessions.
A Meta-analysis of 11 studies (n = 53,378 participants) reported a 2.5% prevalence (95% CI 1.7–3.6%) in developed countries, with no significant gender differences, according to Postlethwaite A. et al. 2019 study titled ” Prevalence of Hoarding Disorder” published in the Journal of Affective Disorder. Individuals with HD exhibit hyper-sentimentality, viewing possessions as extensions of their identity and using items as safety signals to manage emotional regulation challenges.
Did you know most health insurance plans cover mental health treatment? Check your coverage online now.
Why Do People Hoard?
People hoard because of psychological coping mechanisms, childhood experiences, and trauma or loss. Hoarding serves as an emotional coping strategy for stress, anxiety, or feelings of powerlessness, providing a sense of control through acquiring or retaining possessions. Childhood factors like material deprivation, neglect, or witnessing parental struggles with scarcity instill lifelong attachment to belongings as a defense against perceived inadequacy.
Traumatic events such as abuse, bereavement, or relationship breakdowns trigger hoarding as a way to buffer emotional pain or preserve memories linked to lost loved ones. Difficulties with decision-making, perfectionism, and cognitive challenges in organizing items contribute to clutter accumulation.
What is the Difference Between Hoarding and Collecting?
The main difference between hoarding and collecting lies in organization, intent, and emotional impact. Hoarding is a mental health disorder characterized by excessive accumulation of clutter, difficulty discarding items, and emotional distress caused by overwhelming disorganization. Collecting, by contrast, involves the intentional acquisition and systematic organization of specific items (e.g., stamps, antiques) for personal enjoyment or display without clutter or impairment. While collectors take pride in curating and sharing their possessions, hoarders experience shame and isolation due to chaotic living conditions. Hoarding disrupts daily life, whereas collecting remains a controlled hobby that enhances well-being.
What are the Symptoms of Hoarding Disorder?
The symptoms of hoarding disorder are persistent difficulty discarding items, compulsive accumulation of clutter, significant distress avoiding social interactions, disorganization, health hazards, strained relationships, functional impairment in daily tasks and accumulation of items.
This mental health condition involves saving items perceived as valuable or emotionally meaningful, leading to disorganized living spaces that hinder safety and social interactions.
The common symptoms of hoarding disorder are given below
- Persistent difficulty discarding items, even those with low actual value.
- Compulsive accumulation of clutter that impedes the use of living spaces.
- Distress or anxiety when considering disposal of possessions.
- Avoidance of social interactions due to shame about cluttered environments.
- Difficulty organizing or categorizing items.
- Indecisiveness and procrastination in decision-making.
- Health hazards from blocked exits, pest infestations, or unsanitary conditions.
- Strained relationships due to conflicts over clutter management.
- Functional impairment in daily tasks like cooking, cleaning, or bill management.
- Accumulation of items in non-residential spaces (e.g., vehicles, storage units).
What are the Cognitive Symptoms of Hoarding Disorder?
The cognitive symptoms of hoarding disorder are categorization deficits, information-processing challenges, decision-making difficulties, working memory limitations, planning and organization impairments, and visuospatial processing weaknesses.
Approximately 24–30% of HD individuals show clinically significant deficits in visual categorization tasks compared to controls; Mackin, R. S. et al. 2015 study titled “Patterns of Clinically Significant Cognitive Impairment in Hoarding Disorder” published in the Journal of Depression and Anxiety.
Other cognitive domains like episodic memory, language, and visuospatial ability show no significant differences from controls.
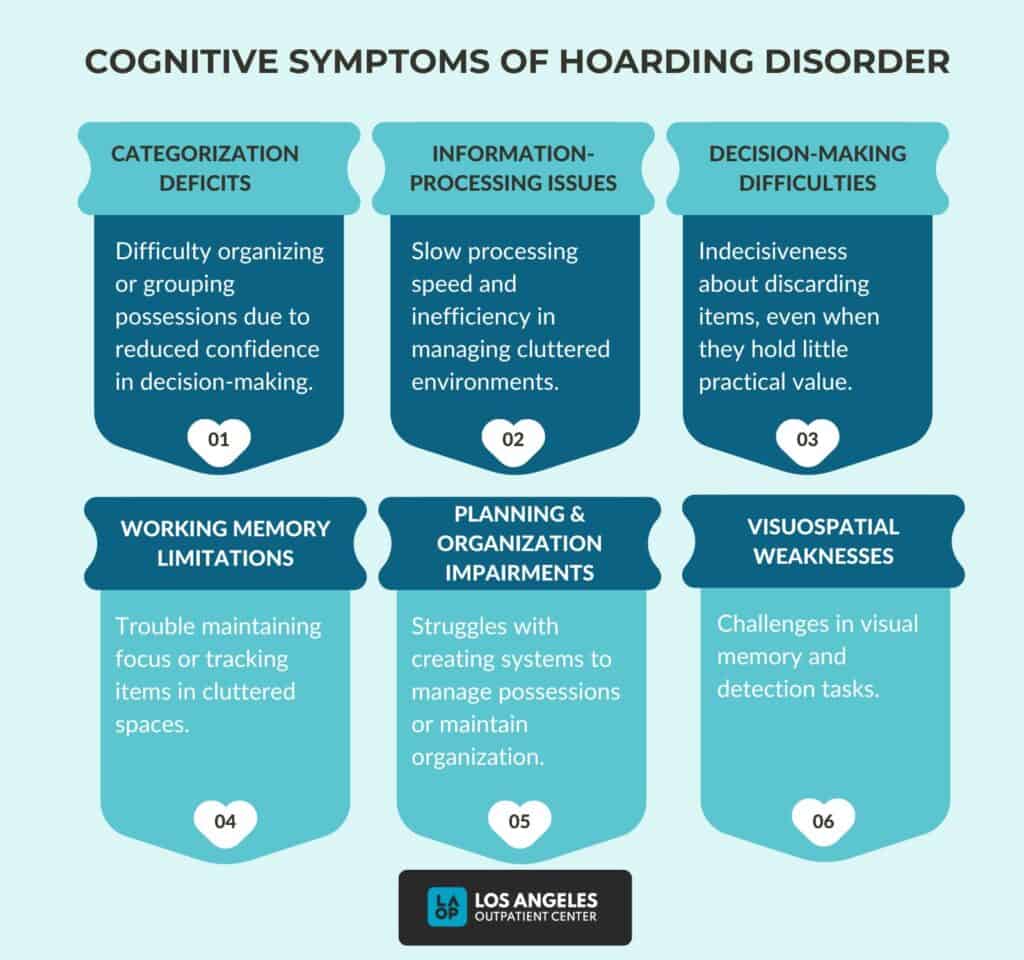
The common cognitive symptoms of hoarding disorder are given below:
- Categorization deficits: Categorization involves difficulty in organizing or grouping possessions due to reduced confidence in decision-making during categorization tasks.
- Information-processing challenges: Slowed processing speed and inefficiency in managing cluttered environments.
- Decision-making difficulties: Indecisiveness about discarding items, even when they hold little practical value.
- Working memory limitations: Reported difficulties in maintaining focus or tracking items in cluttered spaces, though not consistently validated across studies.
- Planning and organization impairments: Struggles with creating systems to manage possessions or maintain organized living spaces.
- Visuospatial processing weaknesses: Potential challenges in visual memory and detection tasks.
What Causes Hoarding Disorder?
The causes of hoarding disorder are genetic predisposition, neurocognitive deficits, emotional attachment to possessions, and environmental influences. Familial patterns, with individuals having a family history of hoarding, are more likely to develop the disorder.
A 2014 study found that 36% of hoarding variance was attributed to genetic factors, with a low genetic correlation (0.10) between hoarding and obsessive-compulsive symptoms, according to Mathews CA et al. ‘s 2014 research, “Partitioning the Etiology of Hoarding and Obsessive-compulsive Symptoms,” published in the Journal of Psychology and Medicine.
Neurocognitive challenges, such as difficulties with decision-making, organization, and executive functioning, are consistently observed. Emotional factors like perfectionism, fear of loss, and avoidance behaviors also play roles, as individuals hoard to cope with stress, trauma, or low self-esteem.
Environmental and psychological triggers further complicate the etiology. Stressful life events (e.g., loss, abuse) or childhood experiences of deprivation or neglect exacerbate symptoms. Additionally, hoarding co-occurs with mental health conditions like depression, anxiety, or OCD, though it is distinct in its symptom profile. Despite advances in understanding these factors, the interplay between biological, psychological, and social elements remains poorly defined, highlighting the need for continued research.
Contact us today to schedule an initial assessment or to learn more about our services. Whether you are seeking intensive outpatient care or simply need guidance on your mental health journey, we are here to help.
Is hoarding genetic?
Yes, hoarding has a significant genetic component, though environmental factors also play a role. Twin studies consistently show heritability estimates ranging from 26% to 50%, with genetic factors accounting for approximately 50% of the variance in compulsive hoarding in female twins, according to Iervolino AC et al.’s 2009 study, “Prevalence and Heritability of Compulsive Hoarding,” published in the American Journal of Psychiatry.
Though heritability decreases slightly with age (41% at 15 vs. 29% in young adulthood), familial clustering persists, with nearly 50% of geriatric hoarding patients reporting affected relatives, according to Dozier, M. E. et al.’s 2017 study, “The Etiology of Hoarding Disorder,” published in the Journal of Psychopathology.
What are the Risk Factors for Hoarding Disorder?
The risk factors for hoarding disorders are brain injury, traumatic life events, impulsive buying habits, substance use disorder and Prader-Willi syndrome.
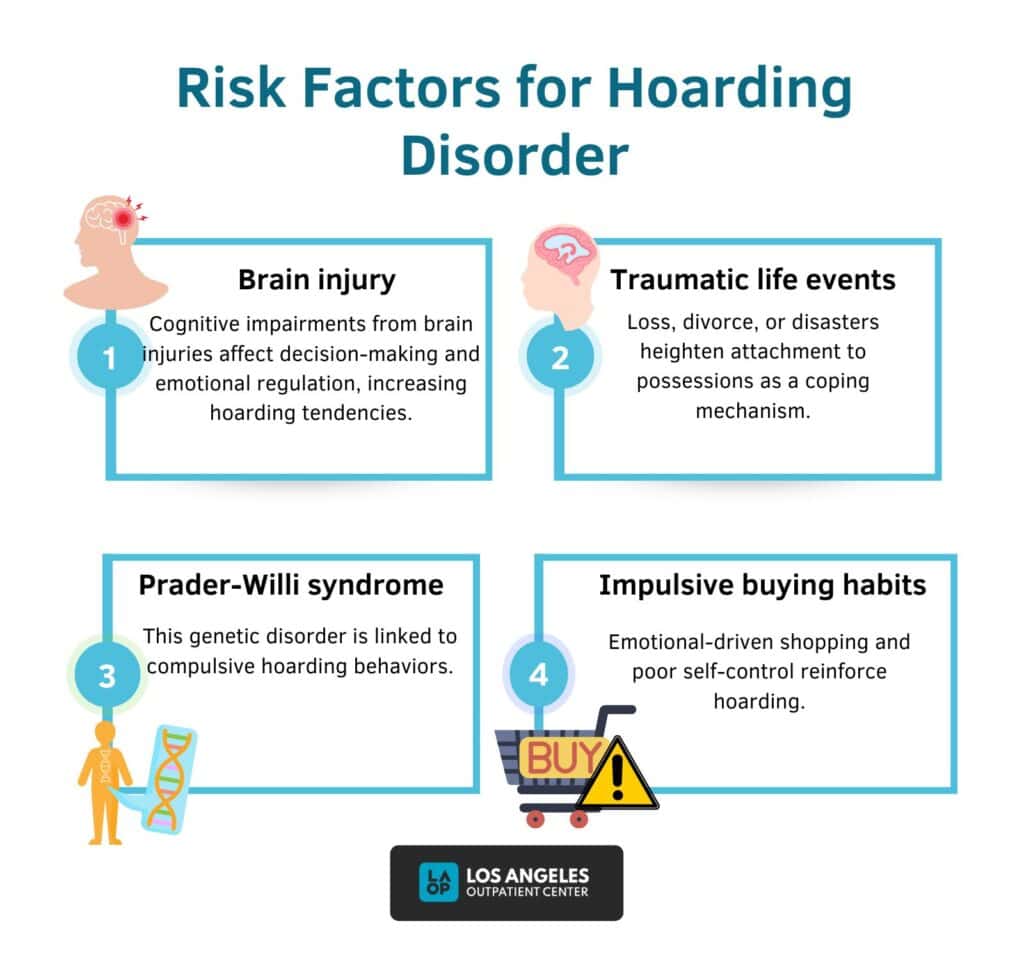
The common risk factors for hoarding disorders include:
- Brain injury: Neuropsychological conditions like brain injuries or dementia contribute to hoarding behaviors due to impaired cognitive functioning, particularly in executive functions (e.g., decision-making, organization). For example, damage to brain regions involved in emotional regulation or memory disrupts standard attachment to possessions. About 26% of individuals with hoarding in the Brain Health Registry reported a history of TBI or concussions, compared to 17.4% without hoarding, according to Vieira, L. S et al. 2022 study titled, “Identifying Psychiatric and Neurological Comorbidities Associated with Hoarding Disorder Through Network Analysis” published in the Journal of Psychiatric Research.
- Traumatic life events: Stressful experiences such as losing a loved one, divorce, eviction, or natural disasters trigger or exacerbate hoarding. These events heighten emotional attachment to possessions as a coping mechanism or create avoidance behaviors related to discarding items. Approximately 71% of participants with late-life hoarding reported symptoms prior to head injury, suggesting hoarding predates or coexist with TBI, according to Ayers, C. R., et al. 2010 study titled, “Age at Onset and Clinical Features of Late Life Compulsive Hoarding” published in the International Journal of Geriatric Psychiatry.
- Prader-Willi syndrome: This genetic disorder is associated with compulsive behaviors, including hoarding. Individuals with Prader-Willi syndrome exhibit rigid attachment to possessions, likely due to neurobiological factors tied to the syndrome. About 37–58% of a cohort with PWS (ages 5–47) displayed hoarding, alongside other compulsive behaviors like ordering objects or repetitive questioning, according to Dykens EM et al.’s 1996 study titled “Obsessions and compulsions in Prader-Willi syndrome” published in the Journal of Child Psychological Psychiatry.
- Impulsive buying habits: Impulsive acquisition of items driven by emotional needs or avoidance of distress reinforces hoarding behaviors. This pattern results from broader difficulties in self-regulation and executive functioning deficits (e.g., indecisiveness, procrastination).
What are the Complications of Untreated Personality Disorders?
The complications of untreated personality disorders are injury, family conflicts, Poor work performance and legal issues, such as eviction. Injury arises from self-harm behaviors (e.g., cutting, suicide attempts) or reckless actions like substance abuse, unsafe sex, or dangerous driving.
Family conflicts and strained relationships result from emotional instability, fear of abandonment, and impulsive communication patterns, potentially leading to isolation or divorce. Poor work performance stems from interpersonal difficulties, mood swings, and impulsivity, increasing the likelihood of job loss or unemployment.
Legal issues include arrests due to substance-related offences, reckless behavior, or violent outbursts, with complications like an eviction from unstable housing situations. Without intervention, these disorders perpetuate cycles of dysfunction, reducing quality of life and increasing societal burdens.
How is Hoarding Disorder Diagnosed?
Hoarding Disorder is diagnosed through a structured clinical evaluation process that assesses persistent difficulty discarding possessions, clutter accumulation, and functional impairment. Clinicians use the DSM-5 criteria, which require persistent difficulty discarding items due to a perceived need to save them and distress during disposal. This leads to cluttered living spaces that compromise their intended use. The diagnosis also mandates clinically significant distress or impairment in social, occupational, or safety domains.
Exclusion criteria rule out hoarding attributable to other medical conditions (e.g., brain injury) or mental disorders (e.g., OCD, schizophrenia). Assessments involve structured interviews about acquisition habits, clutter impact, and daily functioning, alongside collateral information from family/friends and visual documentation of clutter.
Clinicians use rating scales (e.g., Clutter Image Rating Scale) and evaluate for excessive acquisition and insight levels (good, fair, poor, or absent). Poor insight and shame delay self-referral, necessitating third-party interventions. Differential diagnosis distinguishes hoarding from other conditions like depression or autism, ensuring accurate classification.
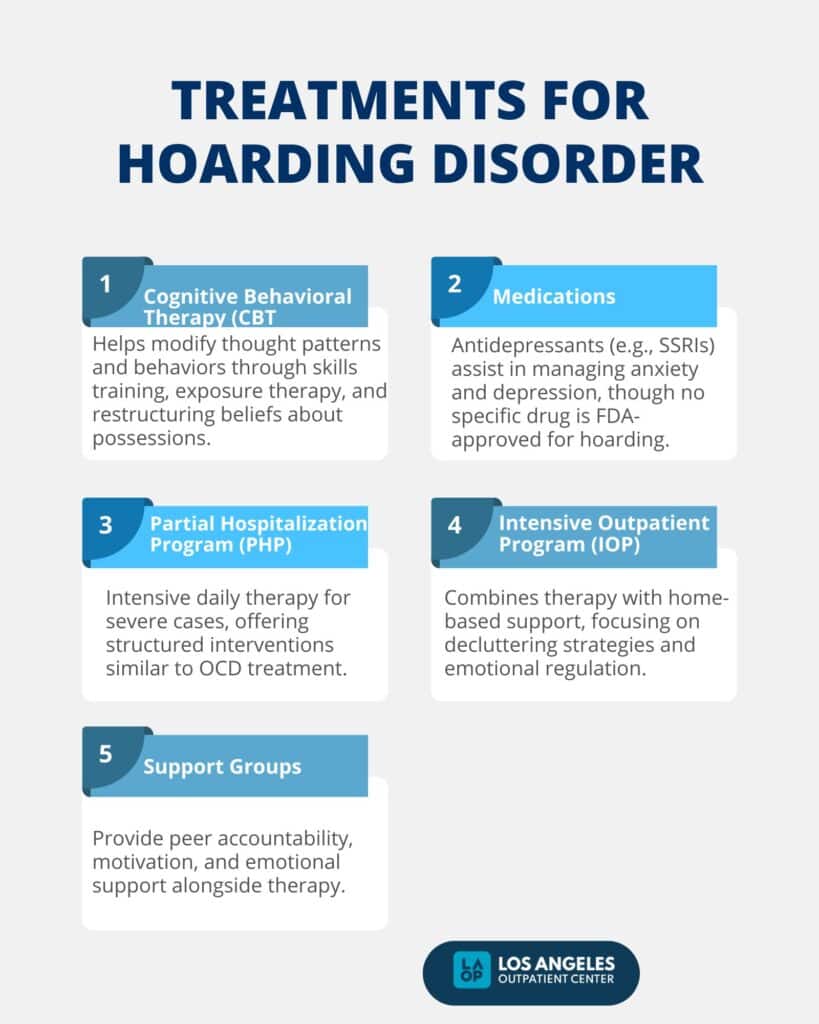
What are the Treatments for Hoarding Disorder?
The treatments for hoarding disorder are cognitive behavioral therapy (CBT), medications, partial hospitalization program (PHP), an intensive outpatient program (IOP) and support groups. These approaches to hoarding disorder treatment aim to help individuals overcome the disorder and improve their overall quality of life.
The treatments for hoarding disorder are listed below.
Cognitive Behavioral Therapy (CBT): CBT addresses hoarding disorder by targeting cognitive distortions and behavioral patterns through structured interventions. It includes skills training (organizing, decision-making), exposure therapy (imagined/direct exposure to discarding), and cognitive restructuring of beliefs about possessions. Home visits and motivational interviewing are integrated.
Studies show 70–80% improvement in symptoms after 9–12 months, with sustained gains post-treatment, according to Kar, N. et al. 2011 research titled, “Cognitive Behavioral Therapy for the Treatment of Post-traumatic Stress Disorder,” published in the Neuropsychiatric Disease and Treatment Journal.
- Medications: Medications (e.g., antidepressants and anti-anxiety drugs) are used adjunctively to manage co-occurring conditions like depression or anxiety, enhancing engagement in therapy. No FDA-approved drugs specifically target hoarding, but SSRIs alleviate symptoms in comorbid cases. A 2013 trial demonstrated a 36% decrease in hoarding severity (UCLA Hoarding Severity Scale) and a 70% response rate in 23 completers after 12 weeks of venlafaxine extended-release, as reviewed by Saxena S et al. 2014 study titled, “Venlafaxine Extended-release Treatment of Hoarding Disorder” published in the International Clinical Psychopharmacology Journal.
- Partial Hospitalization Program (PHP): PHP provides structured, intensive daily therapy (e.g., group sessions, skill-building) for severe cases requiring supervision. It mirrors approaches for OCD and trauma, offering safety-focused interventions. A study of 2,000 patients in acute PHPs (mean stay: 5.3 ± 3.0 days) showed significant improvements in anxiety, depression, hopelessness, and resilience, with effect sizes ranging from Cohen’s d = 0.39 to 1.1, according to Lieberman PB et al. 2017 research titled, “Outcomes of Acute Partial Hospital Treatment” published in the Journal of Psychiatric Practice.
- Intensive Outpatient Program (IOP): IOP combines multiple weekly therapy sessions with home-based support, focusing on decluttering strategies and emotional regulation. Programs emphasize practical skill development and accountability. A 2024 study of 258 adults with PTSD found that IOP participation led to a 56% reduction in inpatient psychiatric hospitalizations (adjusted odds ratio = 0.42, p < 0.01), according to Abeldt BM et al. 2024 study titled “Changes in Service Use After Participation in an Intensive Outpatient Program Among Adults With Posttraumatic Stress Disorder” published in The Permanente Journal.
- Support Groups: Support groups offer peer accountability and emotional validation paired with CBT. They help individuals normalize experiences and maintain motivation during recovery. A 2002 national survey identified 7,467 mutual support groups, self-help organizations (SHOs), and consumer-operated services (COSs) in the U.S., serving 1,005,400 SHO members and 534,551 COS clients annually, according to Goldstrom ID et al. 2006 study titled, “National Estimates for Mental Health Mutual Support Groups, Self-help Organizations, and Consumer-operated Services” according to the journal of Administration and Policy in Mental Health and Mental Health,
Are you covered for treatment?
LAOP is an approved provider for Blue Shield of California and Magellan, while also accepting many other major insurance carriers.
Check Coverage Now!Can hoarding be cured?
No. Hoarding disorder cannot be definitively “cured,” but effective management through specialized cognitive behavioral therapy (CBT) is the primary evidence-based approach. CBT focuses on restructuring beliefs about possessions, improving decision-making skills, and gradually reducing clutter through home-based sessions.
While antidepressants like SSRIs help comorbid conditions (e.g., depression, anxiety), they lack robust evidence for directly treating hoarding. Treatment success depends on long-term commitment, with relapse prevention strategies required.
How to Help a Loved One with Hoarding Disorder?
To help loved ones with hoarding disorder, approach the situation with compassion and understanding, recognizing that hoarding is a mental health condition rather than a choice. Educate yourself about the disorder to dispel stigma and grasp its emotional roots, such as intense attachment to possessions or fear of loss. Encourage professional help, particularly cognitive behavioral therapy (CBT), the most effective treatment for addressing underlying beliefs and behaviors. Use respectful communication, avoiding judgmental language like “junk” and instead expressing concerns using “I” statements (e.g., “I worry about safety”).
Support harm-reduction strategies prioritizing safety and well-being over total decluttering, such as creating a harm-reduction team with therapists and family members. Avoid unilateral cleanup efforts, as sudden removal of items exacerbates distress; instead, collaborate on small, incremental steps when the individual is ready. Prioritize your mental health through therapy or support groups, as caregiving is emotionally taxing. Explore family-focused interventions like Family-As-Motivators Training to improve communication and reduce conflict.
At What Age Does Hoarding Disorder Start?
Hoarding disorder begins with symptoms emerging between ages 10 and 20, with the median age of onset for core symptoms (saving, difficulty discarding, clutter) falling within this range, according to Bratiotis, C. et al. ‘s 2021 research titled “Hoarding Disorder Development in Conceptualization, Intervention, and Evaluation” published in the Focus: Journal of Lifelong Learning in Psychiatry.
The median age for meeting full diagnostic criteria (simultaneous presence of all three symptoms) is 20–30 years, The median age for meeting full diagnostic criteria of hoarding disorder (simultaneous presence of all three symptoms) is 20–30 years, according to Dozier, M. E. et al. 2015 study titled, “Age of Onset and Progression of Hoarding Symptoms in Older Adults With Hoarding Disorder” published in the Aging & Mental Health Journal. While most cases start early, approximately 23% of older adults report symptom onset after age 40, linked to significant life changes like retirement or loss.
Is Hoarding Disorder More Common in Males or Females?
Hoarding disorder is more common in males than females. A 2022 analysis of clinical data found men are nearly twice as likely to develop hoarding behaviors, with earlier symptom onset compared to women, according to Samuels, J. F. et al. ‘s 2008 research titled “Sex-Specific Clinical Correlates of Hoarding in Obsessive-Compulsive Disorder,” published in the Journal of Behaviour Research and Therapy. However, hoarding disorder does not discriminate based on gender and affects anyone regardless of their sex.
What Items Do People Most Commonly Hoard in Hoarding Disorder?
The items that people most commonly hoard in hoarding disorder are newspapers and magazines, books, clothes, leaflets and letters, junk mail, bills and receipts, containers, including plastic bags and cardboard boxes, household supplies, and animals.
The items that people most commonly hoard in hoarding disorder are:
- Newspapers and magazines
- Books
- Clothes
- Leaflets and letters (including junk mail)
- Bills and receipts
- Containers (plastic bags, cardboard boxes)
- Household supplies
- Animals ( cats, dogs, or other pets)
Is Hoarding a Mental Disorder?
Yes. Hoarding Disorder (HD) is recognized as a distinct mental disorder in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5), characterized by persistent difficulty discarding possessions, cluttered living spaces, and significant distress or functional impairment. It is classified under Obsessive-Compulsive and Related Disorders but is distinct from obsessive-compulsive disorder (OCD), as most individuals with HD lack OCD’s hallmark obsessions or compulsions.
The DSM-5 criteria specify that HD cannot be better explained by other conditions (e.g., brain injury, autism), and research identifies cognitive deficits, emotion regulation challenges, and genetic correlations as contributing factors. About 58% of adults with HD have comorbid mental disorders (e.g., depression, anxiety), according to Nordsletten AE et al. 2013 study titled “Epidemiology of Hoarding Disorder,” published in the British Journal of Psychiatry.
What Mental Health Conditions are Commonly Associated With Hoarding Disorder?
The mental health conditions that are commonly associated with hoarding disorder include obsessive-compulsive disorder (OCD), obsessive-compulsive personality disorder (OCPD), attention-deficit/hyperactivity disorder (ADHD), depression, dementia and schizophrenia.
The mental health conditions that are commonly associated with hoarding disorder include:
Obsessive-compulsive disorder (OCD)
OCD is characterized by intrusive thoughts (obsessions) and repetitive behaviors (compulsions). Approximately 20% of individuals with HD meet the obsessive-compulsive disorder criteria, driven by fears of contamination or catastrophic consequences if items are discarded, according to Frost RO et al. 2011 study titled “Depression Anxiety,” published in the Epub Journal. Hoarding in OCD involves rigid organizing rituals or hyperfocus on symmetry, contrasting with HD’s core difficulty in discarding due to emotional attachment.
Obsessive-Compulsive Personality Disorder (OCPD)
OCPD involves rigid perfectionism, excessive orderliness, and a preoccupation with details. Hoarding in OCPD stems from beliefs about avoiding waste or future utility, which are justified as rational rather than emotional. Unlike HD, OCPD-related hoarding lacks distress about clutter but still disrupts daily functioning through inflexible saving habits.
Attention-deficit/hyperactivity disorder (ADHD)
ADHD is marked by inattention, impulsivity, and executive dysfunction. Approximately 28% of HD cases involve attention-deficit/hyperactivity disorder, where disorganization and impulsive acquisition contribute to clutter, according to Frost RO et al. 2011 study titled “Depression Anxiety,” published in the Epub Journal. ADHD-related hoarding lacks the emotional attachment seen in HD but shares challenges in task planning and decision-making.
Depression
Major depressive disorder (MDD) affects up to 50% of HD cases, manifesting as low motivation, social withdrawal, or emotional numbing, according to Nutley, S.et al. ‘s 2023 study, “Relationship of Hoarding and Depression Symptoms in Older Adults,” published in the American Journal of Geriatric Psychiatry. Depression worsens hoarding by reducing energy for organizing or seeking help, while hoarding exacerbates isolation and self-neglect.
Dementia
Dementia involves progressive cognitive decline, including memory loss and impaired judgment. While not explicitly detailed in the provided studies, dementia-related hoarding stems from confusion, forgetfulness, or loss of executive function, complicating care and safety in cluttered environments.
Schizophrenia
Delusions, hallucinations, and disorganized thinking characterize schizophrenia. Hoarding in schizophrenia involves passive accumulation due to apathy or cognitive deficits, differing from HD’s active saving driven by emotional attachment.
Share This Post

TREATMENTS WE OFFER
Are you covered for treatment?









LAOP is an approved provider for Blue Shield of California and Magellan, while also accepting many other major insurance carriers.
Check Coverage Now!