Excoriation Disorder/ Dermatillomania/ Skin-picking Disorder: Symptoms, Causes, and Treatment

Dermatillomania manifests itself through the compulsive behavior of picking at one’s skin. This behavior often damages tissue and disrupts the individual’s daily life. It affects approximately 2% to 5% of adolescents and adults, with a higher prevalence among females, according to Grant JE et al.’s 2020 study “Prevalence of Skin Picking (excoriation) Disorder,” published in the Journal of Psychiatric Research.
The primary symptom of dermatillomania is the uncontrollable urge to pick at the skin, manifesting as scratching, squeezing, or rubbing. This behavior leads to visible sores, bruises, or scarring. Individuals experience significant distress or embarrassment about their behavior and often attempt to stop but find it difficult.
The exact cause of Dermatillomania is unknown but linked to genetic, environmental, and psychological factors; according to Okumuş, H. G., & Akdemir, D’s 2023 study about Body-Focused Repetitive Behavior Disorders, individuals with a family history of obsessive-compulsive disorder (OCD) or body-focused repetitive behaviors (BFRBs) may have a higher risk of developing this disorder.
Dermatillomania is diagnosed based on the individual’s symptoms and behavior patterns. A mental health professional will conduct an evaluation and use criteria from the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) to make a diagnosis.
What is Excoriation Disorder (Dermatillomania)?
Excoriation Disorder (dermatillomania) is a mental health condition characterized by the compulsive urge to pick at one’s skin, leading to significant tissue damage, according to Anderson S et al.’s 2022 review titled “The Problem With Picking,” published in the Journal of Psychology and Psychotherapy.
This behavior results in visible lesions, infections, and scarring, often causing emotional distress and impairment in daily functioning. Individuals pick at healthy skin or minor imperfections, and the behavior is chronic, with varying periods of intensity.
Historically, dermatillomania was classified under impulse control disorders, according to Dr P S Katharine’s 2023 article, “Excoriation (Skin-Picking) Disorder,” published in the MSD Manual Professional Version Journal. However, with the publication of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), it was reclassified as a distinct condition under the category of Obsessive-Compulsive and Related Disorders. It is officially termed “excoriation (skin-picking) disorder” and is identified by the code L98.1 in the ICD-10.
The DSM-5 criteria for diagnosing Excoriation (Skin Picking) Disorder include several important components. Firstly, there must be recurrent skin picking that results in noticeable lesions. Secondly, individuals must have repeatedly attempted to decrease or stop this behavior.
The condition causes significant distress or impairment in various areas of functioning, such as social or occupational settings. Notably, the behavior cannot be attributed to the physiological effects of a substance or another medical condition, ensuring that the diagnosis is specific and accurate.
According to Grant JE et al.’s 2020 study on “Prevalence of Skin Picking (excoriation) Disorder,” published in the Journal of Psychiatric Research, between 1.4% and 5.4% of adults may be affected by excoriation disorder, with a higher prevalence observed among women than men; however, recent research shows that about 55% of those diagnosed are female. The onset typically occurs during adolescence, around ages 13-15, but can manifest at any age.
This disorder often co-occurs with other mental health conditions, such as obsessive-compulsive disorder (OCD) and body dysmorphic disorder (BDD), further complicating its prevalence and treatment outcomes.
Did you know most health insurance plans cover mental health treatment? Check your coverage online now.
Is Dermatillomania a Form of Self-harm?
No. Dermatillomania, or skin-picking disorder, is not classified as self-harm in the traditional sense. However, it shares some similarities with self-harming behaviors, according to N Fugen et al. ‘s 2001 article, “Skin Picking as a Form of Self-Injurious Behavior,” published in the ResearchGate Journal.
Self-harm is defined as the conscious decision to inflict injury on oneself without suicidal intent. This behavior is often associated with emotional distress, where individuals may seek to relieve psychological pain through physical pain.
According to the DSM-5, self-harm is categorized as non-suicidal self-injury (NSSI). It involves a deliberate action to harm oneself, as reviewed by Klonsky ED et al.’s 2014 study “Nonsuicidal self-injury: what we know, and what we need to know, published in the Canadian Journal of Psychiatry.
In contrast, dermatillomania is recognized as a type of body-focused repetitive behavior (BFRB) and is classified under obsessive-compulsive disorder. Individuals with dermatillomania start picking their skin consciously but often transition into an unconscious habit that can cause significant skin damage and emotional distress.
Unlike self-harmers, skin pickers typically do not seek pain; instead, they experience a sense of relief or even pleasure during the act of picking.
According to Priusha Ravipati from the Department of Drug Sciences, University of Pavia, those who engage in self-harm are usually aware of their actions and the pain they are inflicting. At the same time, individuals with dermatillomania may not recognize their behavior as harmful until it has escalated.
While dermatillomania involves harmful behaviors similar to self-harm, it is classified differently due to its underlying psychological mechanisms and the nature of the actions involved.
Is Dermatillomania an Anxiety Disorder?
Yes, dermatillomania, also known as excoriation disorder, is classified under the category of obsessive-compulsive and related disorders in the DSM-5, according to Malayala SV et al.’s 2021 study titled “A Case Report and Literature Review, published in the Journal of Psychiatric Research.
It is characterized by repetitive skin picking that leads to tissue damage and significant distress or impairment in functioning.
Dermatillomania is closely linked to anxiety disorders. Individuals with this condition often experience heightened anxiety, shame, and depression due to the visible effects of their skin picking.
According to Grant JE et al.’s 2020 study titled “Prevalence of Skin Picking (excoriation) Disorder,” published in the Journal of Psychiatric Research, a significant percentage of those with dermatillomania also have comorbid anxiety disorders, such as generalized anxiety disorder, with rates reported as high as 63.4%.
Anxiety acts as a trigger for skin-picking behaviors. Many individuals use skin picking as a coping mechanism to manage feelings of stress or anxiety. This behavior may temporarily relieve negative emotions but ultimately leads to further distress and a cycle of picking. Common triggers include stressful situations, negative emotions, and inactivity or boredom.
While dermatillomania itself is not classified solely as an anxiety disorder, it is significantly influenced by anxiety, which can exacerbate the condition and complicate treatment efforts.
Is Dermatillomania OCD?
Yes. Dermatillomania is associated with obsessive-compulsive disorder (OCD), according to Khatib HA et al.’s 2022 study titled “Prevalence of and Risk Factors for Skin Picking Disorder Symptoms Among Adults in an Arab Middle Eastern Population” published in the Journal of Clinical, Cosmetic and Investigational Dermatology.
Both disorders involve compulsive behaviors, yet they manifest differently and stem from varying underlying motivations.
Dermatillomania is characterized by the repetitive and uncontrollable act of picking at the skin, which leads to tissue damage and emotional distress. OCD is driven by intrusive thoughts that compel individuals to perform certain behaviors to alleviate anxiety or prevent perceived adverse outcomes.
According to Khatib HA’s study, individuals with dermatillomania are more likely to have OCD or related disorders than those without skin-picking issues. While both conditions involve compulsive actions, the motivations differ: individuals with OCD pick their skin to eliminate perceived dirt or contaminants.
Treatment approaches for both conditions also share similarities but require tailored strategies. Cognitive Behavioral Therapy (CBT) is effective for both dermatillomania and OCD, focusing on changing maladaptive thought patterns and behaviors.
While dermatillomania and OCD are interconnected through their compulsive nature and shared treatment modalities, they are distinct disorders with different underlying motivations and manifestations.
Is Dermatillomania ADHD?
No. Dermatillomania is not classified as ADHD, but there is a notable connection between the two, according to Grant JE et al.’s 2021 review of “Trichotillomania and Skin-Picking Disorder,” published in The Journal of Lifelong Learning in Psychiatry.
Individuals with ADHD often exhibit impulsive behaviors, which include skin picking. The underlying mechanisms differ between dermatillomania and ADHD, yet the impulsivity associated with ADHD increases the likelihood of developing skin-picking habits.
ADHD is characterized by impulsivity and hyperactivity, which leads to behaviors such as skin picking as a form of self-soothing or stimulation.
Individuals with ADHD often experience sensory processing issues. Skin picking is a coping mechanism to either alleviate overstimulation or provide stimulation when feeling understimulated.
Dermatillomania is classified as a body-focused repetitive behavior (BFRB) rather than an obsessive-compulsive disorder (OCD). While OCD involves intrusive thoughts leading to compulsive actions aimed at reducing anxiety (such as excessive hand washing), dermatillomania primarily centers around the obsessive act of picking skin without necessarily being linked to intrusive thoughts.
In OCD, compulsions are often performed in response to specific obsessions (e.g., fear of contamination). In contrast, individuals with dermatillomania pick their skin due to boredom, anxiety relief, or sensory needs rather than specific worries.
While dermatillomania is not ADHD, the impulsivity and sensory processing challenges inherent in ADHD lead to an increased propensity for skin-picking behaviors. Understanding this relationship is crucial for effective treatment strategies that simultaneously address both conditions.
What Are the Symptoms of Dermatillomania?
The symptoms of dermatillomania are physical, behavioral, and psychological, including skin picking, scarring, and feelings of anxiety, as reviewed by Dr Jeanne M. Fama’s article “What is Skin Picking Disorder?” in the International OCD Foundation Journal.

Below are the symptoms of dermatillomania according to the International OCD Foundation Journal:
Contact us today to schedule an initial assessment or to learn more about our services. Whether you are seeking intensive outpatient care or simply need guidance on your mental health journey, we are here to help.
Physical Symptoms of Dermatillomania
Physical symptoms are those that affect the appearance of the skin and include:
- Redness and inflammation: Constant picking at the skin causes redness and inflammation, making it look irritated.
- Scabs and sores: Picking at the same spot repeatedly leads to scabs or open sores.
- Bruising: Intense picking results in bruising on the affected area.
- Bleeding: Aggressive picking causes bleeding from the picked area.
- Skin lesions: Chronic skin picking permanently damages the skin, leading to visible scars, cuts, or indentations.
The physical symptoms of dermatillomania vary and may be more severe in some individuals than others. Seeking professional help is crucial in managing these symptoms and preventing further damage to the skin.
Behavioral Symptoms of Dermatillomania
Behavioral symptoms are the actions or behaviors that are associated with dermatillomania and include:
- Picking at the skin: The most common behavioral symptom of dermatillomania is the constant picking, scratching, or squeezing of the skin.
- Preoccupation with perceived imperfections: People with this disorder may constantly search for flaws or blemishes on their skin to pick at.
- Use of tools: Some individuals may use tweezers or needles to pick up their skin.
- Hiding behavior: Many people with dermatillomania feel ashamed and embarrassed about their picking and may try to hide it from others.
These behavioral symptoms are not a choice and are often uncontrollable urges. Seeking treatment helps manage these behaviors and improve overall mental health.
Psychological Symptoms of Dermatillomania
Psychological symptoms are related to a person’s thoughts, feelings, and emotions and include:
- Feelings of anxiety: Many people with dermatillomania experience feelings of fear, tension, or stress before and during skin picking.
- Relief from picking: Despite the negative consequences, some individuals feel a sense of relief or pleasure after picking their skin.
- Guilt or shame: The cycle of picking followed by temporary relief can lead to guilt and shame for many individuals.
- Negative impact on self-esteem: Constantly picking at one’s skin can lead to a negative body image and low self-esteem.
These symptoms are not always present in every individual with dermatillomania, and the severity of symptoms may vary. It is important to seek professional help if these symptoms are causing distress or interfering with daily life.
What Are Different Types of Skin Picking?
The different types of skin picking are automatic and focused picking, according to Jafferany et al.’s 2019 post titled “Skin-Picking Disorder,” published in the CNS Drugs Journal.
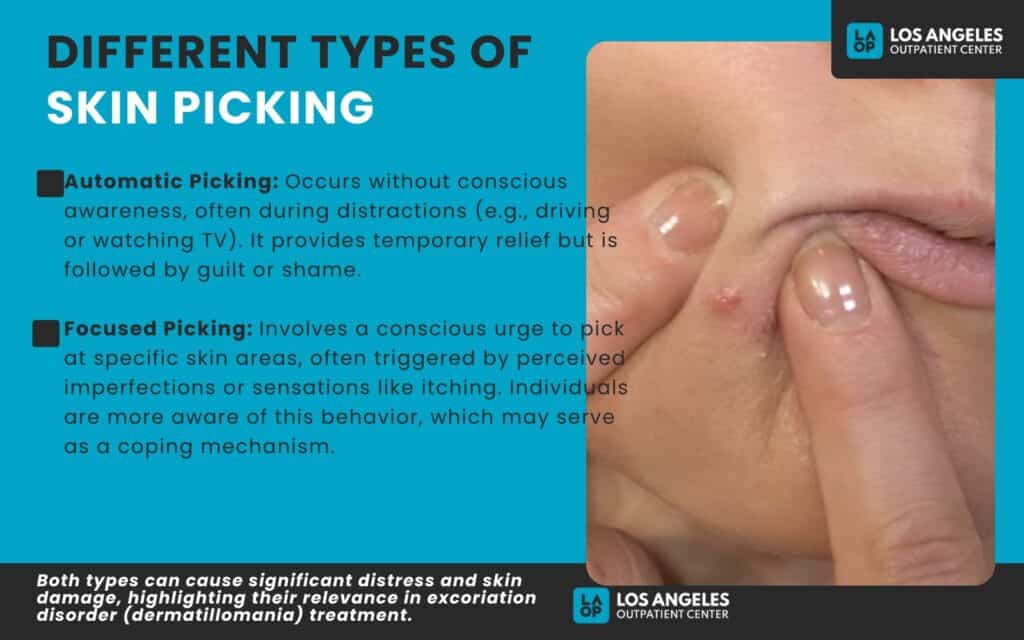
- Automatic Picking: This type of skin picking occurs without conscious awareness. Individuals use automatic picking while distracted, such as driving, watching TV, or reading. It is often described as a form of self-stimulation, where the person experiences a sense of relief while picking, followed by feelings of guilt or shame afterward.
- Focused Picking: Unlike automatic picking, focused picking is characterized by a conscious urge to pick at specific areas of the skin. This behavior is often triggered by perceived imperfections, such as scabs or blemishes, or by physical sensations like itching. Individuals are typically more aware of their actions during focused picking and may use it as a coping mechanism to alleviate discomfort or boredom.
Both types of skin picking lead to significant distress and physical damage to the skin, highlighting the importance of understanding these behaviors within the context of excoriation disorder (dermatillomania) and its treatment options.
What Causes Excoriation Disorder?
The causes of excoriation disorder are biological and are categorized into three main factors: biological, psychological, and environmental, according to Farhat LC et al.’s 2023 review titled “A Systematic Review and Meta-Analysis,” published in the Journal of Psychiatry.
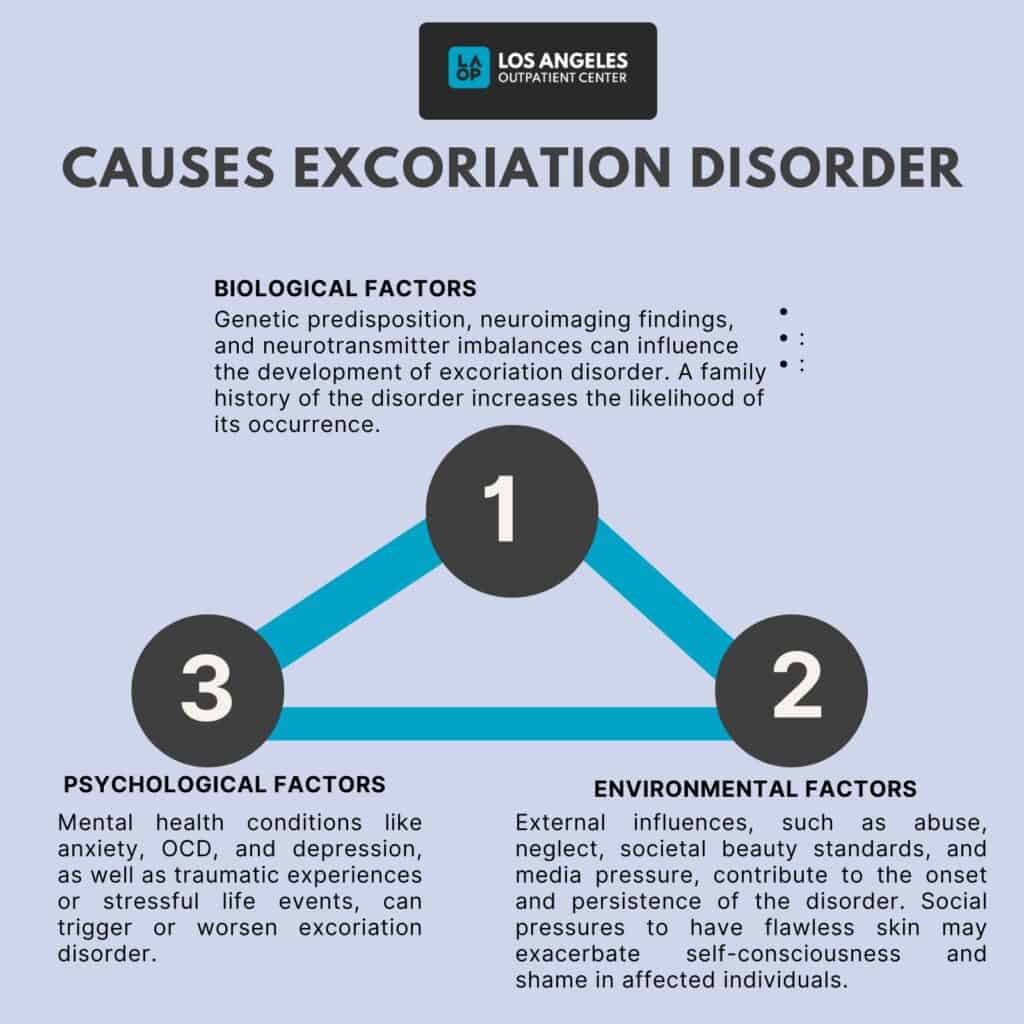
The following are the 3 causes of excoriation disorder, according to the Journal of Psychiatry.
- Biological Factors: Biological factors are the factors that directly influence the development of excoriation disorder. These factors include genetics, neuroimaging, and neurotransmitter abnormalities. According to Okan Ibiloğlu A et al.’s 2016 study “A Case of Skin Picking Disorder of a Patient with a History of Childhood Abuse,” published in the Archives of Neuropsychiatry Journal, individuals with a family history of excoriation disorder are more likely to develop the disorder themselves.
- Psychological Factors: Psychological factors refer to the mental and emotional aspects that may contribute to the development of excoriation disorder. These include underlying mental health issues such as anxiety, OCD, or depression, as reviewed by Murayama K’s 2020 study titled “Impacts of Stressful Life Events and Traumatic Experiences on Onset of Obsessive-Compulsive Disorder,” published in the Front Psychiatry Journal, traumatic experiences or stressful life events trigger the onset of excoriation disorder in some individuals.
- Environmental Factors: Environmental factors are external influences that can contribute to developing and maintaining excoriation disorder. These include a history of abuse or neglect, peer pressure, societal beauty standards, and media influence.
In a society where there is immense pressure to have flawless skin and perfect appearance, individuals with excoriation disorder feel even more self-conscious and ashamed.
Therefore, combining these factors plays a role in the development of excoriation disorder. It is essential to understand that this disorder is not caused by personal weakness or character flaws but rather by a complex interplay of biological, psychological, and environmental factors.
Are you covered for treatment?
LAOP is an approved provider for Blue Shield of California and Magellan, while also accepting many other major insurance carriers.
Check Coverage Now!Can Medications Cause Skin-Picking?
Yes, medications trigger or worsen skin-picking behaviors, including dermatillomania. Lamotrigine, an anticonvulsant often used to treat epilepsy and bipolar disorder, has been studied for its effects on pathologic skin picking.
According to Grant JE et al.’s 2007 study “Lamotrigine Treatment of Pathologic Skin Picking” in the Journal of Psychiatry, while lamotrigine helps to reduce symptoms in some individuals with dermatillomania, its efficacy is not universally accepted. In a study involving 24 participants, significant reductions in the time spent picking were observed, with about two-thirds reporting improvement.
While some patients experience a reduction in their urges to pick at their skin, others find that their symptoms worsen or remain unchanged. This variability is attributed to individual differences in brain chemistry and the underlying mental health conditions associated with dermatillomania, such as anxiety or obsessive-compulsive disorder (OCD).
How is Excoriation Disorder Diagnosed?
Excoriation Disorder, commonly known as skin-picking disorder (SPD), is diagnosed through a structured process that includes clinical criteria as outlined in the DSM-5, as well as self-reporting and behavioral assessments, according to Snorrason I et al.’s 2022study “Assessing Excoriation (Skin-Picking) Disorder” published in the Environmental Research and Public Health Journal.
In the clinical criteria, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) specifies several criteria that must be met for a diagnosis of Excoriation Disorder: There must be recurrent skin picking, attempts to reduce skin picking, and distress or impairment in social areas of functioning. There must also be the exclusion of other causes where skin picking cannot be attributed to another medical condition.
Skin Picking Disorder (SPD) assessment extends beyond the DSM-5 criteria to include various self-reporting tools and behavioral evaluations that comprehensively understand the disorder.
One such tool is the Diagnostic Interview for Skin Picking Problems (DISP), a semi-structured interview designed to evaluate both DSM-5 criteria and clinical features of SPD, including the frequency and duration of picking episodes; it has demonstrated good reliability and validity in clinical settings.
The diagnosis of Excoriation Disorder involves a comprehensive approach that combines established clinical criteria from the DSM-5 with structured interviews and self-report measures.
Can You Self-diagnose Dermatillomania?
Yes, you can self-diagnose dermatillomania to some extent. Still, it is not advisable to rely solely on self-assessment, according to Jenkins Z et al.’s review, “Should Skin Picking Disorder be Considered a Diagnostic Category?” published in the Australian and New Zealand Journal of Psychiatry.
Self-assessment tools for dermatillomania, or skin-picking disorder, include several online quizzes designed to help individuals evaluate their symptoms. Notable options are the ADDitude Self-Test, which is based on DSM-5 criteria for both children and adults; the SkinPick.com Assessment, which measures the severity of skin-picking behaviors using established psychometric scales; and the OCD Center of Los Angeles Test, developed from clinical experience to identify compulsive skin-picking behaviors.
While these self-tests provide valuable insights, they are not definitive diagnostic tools. Self-diagnosis carries risks such as misinterpretation of symptoms, overlooking other mental health conditions like anxiety or depression, and a lack of professional guidance that could offer tailored advice and support.
Seeking professional help ensures a comprehensive evaluation and access to appropriate treatment strategies. Discussing concerns with a qualified mental health professional, regardless of self-test results, is crucial.
Should You Go to a Dermatologist if You Have Dermatillomania?
Yes, you can visit a dermatologist if you have dermatillomania, especially when the condition leads to significant skin damage or emotional distress, according to Malayala SV et al.’s 2021 post “A Case Report and Literature Review. Cureus” published in the Cureus Journal of Medical Sciences.
Seeing a dermatologist is important, particularly when experiencing severe skin damage, such as open wounds or scarring, which require specialized wound care and scar management options like laser therapy.
Dermatologists address underlying skin conditions, such as acne or eczema, worsening the urge to pick. It is crucial to find a dermatologist who understands the psychological aspects of dermatillomania, as effective treatment often involves collaboration with mental health professionals.
These specialists prescribe medications, including topical treatments and SSRIs, and suggest therapies like cognitive-behavioral therapy (CBT) to help manage the behavioral components of the disorder. A holistic approach that considers physical and psychological factors is ideal, as it allows for developing coping strategies and understanding triggers.
Common Misdiagnoses: Overlapping with BFRBs
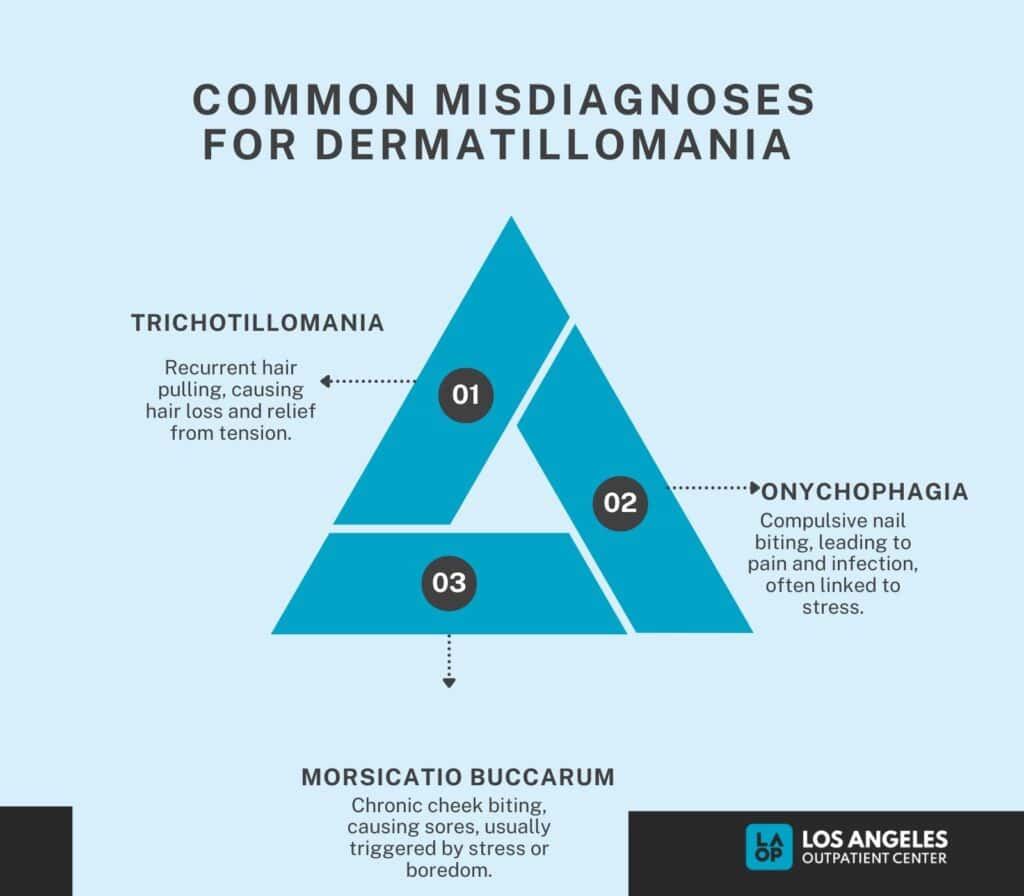
The common misdiagnoses for dermatillomania include hair pulling, nail-biting, and cheek biting, According to Snorrason I et al.’s 2012 review titled, “Skin Picking Disorder is Associated With Other Body-focused Repetitive Behaviors” published in the Ann Clinical Psychiatry Journal.
Excoriation disorder is misdiagnosed due to its overlap with other body-focused repetitive behaviors like nail-biting and cheek-biting. This leads healthcare providers to misinterpret the symptoms as manifestations of other disorders within the OCD spectrum or even as simple grooming habits, resulting in inadequate treatment strategies.
Common misdiagnosed disorders include:
- Trichotillomania (Hair Pulling Disorder): Hair pulling is characterized by recurrent pulling out of one’s hair, leading to noticeable hair loss. Individuals pull hair from the scalp, eyebrows, or other areas, often feeling tension before pulling and relief afterward.
- Onychophagia (Nail Biting): Nail biting involves compulsive biting of the nails and surrounding skin, which results in pain and infection. This behavior often serves as a coping mechanism for stress or anxiety.
- Morsicatio Buccarum (Cheek Biting): Check biting refers to the chronic biting of the inside of the cheeks, which causes sores and discomfort. This behavior is often unconscious and occurs during stress or boredom.
Differentiating these disorders from excoriation disorders is crucial for effective treatment.
Rediscover Life at Los Angeles Outpatient Center
Get the compassionate mental health support you deserve. We're here to help you reclaim joy, wellness, and a brighter future.
Our Facility
What Are Treatment Options for Dermatillomania?
The treatment options for dermatillomania include cognitive behavioral therapy, medications, and natural remedies.
1. Cognitive Behavioral Therapy (CBT)
CBT is the primary psychological intervention for dermatillomania. It focuses on altering the thought patterns that contribute to skin picking. It helps individuals understand their behavior’s triggers and emotional states, enabling them to develop healthier coping mechanisms.
Habit reversal integrates into CBT and involves two main components: awareness and competing response training. This method teaches individuals to identify early signs of skin picking and replace the behavior with healthier alternatives.
According to Revankar RR et al. ‘s 2022 study “Cognitive Behavior Therapy as Dermatological Treatment” in the Journal of Women’s Dermatology, patients undertaking cognitive behavioral therapy also reported a 77% reduction in skin picking from the pretreatment period, while the wait-listed control group only had a 16% decrease.
2. Medications
Medications used to treat excoriation disorder include antidepressants or antipsychotics to help manage the underlying psychological issues that contribute to dermatillomania. These medications help reduce anxiety, depression, and obsessive-compulsive symptoms often present in individuals with skin-picking disorder. According to Chouinard G. et al.’s 1992 study titled, “Sertraline in the Treatment of Obsessive-Compulsive Disorder. According to Chouinard G. et al.’s 1992 study titled “Sertraline in the Treatment of Obsessive-Compulsive Disorder, there was a 52% reduction in compulsive skin-picking behavior and a 30% decrease in depressive symptoms over 16 weeks of study.
3. Natural Remedies and At-home Treatments
Aside from traditional therapy and medication, natural remedies and at-home treatments help individuals with dermatillomania manage their symptoms. These include relaxing techniques such as deep breathing or meditation, using fidget toys to keep hands busy, and keeping a journal to track triggers and emotions.
Natural approaches are effective complementary strategies alongside professional treatment. While they may not replace formal therapies, many find that self-care routines significantly help manage symptoms.
Does Marijuana Help Dermatillomania?
Yes, marijuana has potential benefits for managing symptoms of dermatillomania. Still, the evidence is limited and mixed, according to Dhadwal G et al.’s 2018 article “The Risks and Benefits of Cannabis in the Dermatology Clinic,” published in the Journal of Cutaneous Medicine and Surgery.
Marijuana helps alleviate anxiety, which is a trigger for skin-picking behaviors. Since dermatillomania often coexists with anxiety disorders, managing anxiety might indirectly reduce the urge to pick.
Regular use of marijuana leads to dependency issues, which may complicate the management of dermatillomania and associated mental health conditions.
While there are claims that marijuana helps in managing symptoms of dermatillomania through anxiety reduction and pain relief, the lack of robust research and potential risks necessitate caution. Consulting with a healthcare provider is essential for anyone considering this option as part of their treatment plan.
Can skin-picking disorder be cured?
No, skin-picking disorder is not considered curable in the traditional sense but is manageable, according to LeBlanc MA et al.’s 2024 study, “A Case Report of an Atypical Severe Case of Skin Picking Disorder Managed by a Multidisciplinary Team,” published in BMC Psychiatry Journal. This condition falls under the category of obsessive-compulsive and related disorders and frequently co-occurs with other mental health issues such as anxiety and depression.
Although many individuals can achieve significant improvement through therapy and medication, the disorder often persists over time, leading to periods of remission followed by relapses. Therefore, ongoing management strategies are essential for maintaining progress.
Did you know most health insurance plans cover mental health treatment? Check your coverage online now.
How to Stop Dermatillomania?
To stop dermatillomania, identify triggers, use Cognitive Behavioral Therapy (CBT), practice stimulus control, have a scheduled picking time, exercise emotion regulation techniques, and seek professional help, according to Malayala SV et al.’s 2021 study “A Case Report and Literature Review” published in the Cureus Journal of Medicine.
The following ways are effective in stopping dermatillomania.

- Identify Triggers: Recognize situations, emotions, or thoughts that lead to skin picking. Keeping a journal can help track patterns and identify specific triggers related to stress, anxiety, or boredom.
- Cognitive Behavioral Therapy (CBT): Engage in CBT to learn techniques for modifying thoughts and behaviors associated with skin picking. This therapy can help develop coping strategies and reduce the compulsion to pick.
- Stimulus Control: Modify your environment to reduce triggers. For example, avoid mirrors or tools that facilitate picking, and wear gloves or bandages on fingers to limit access to skin
- Emotion Regulation Techniques: Practice relaxation techniques like deep breathing or progressive muscle relaxation to manage emotions that trigger picking. These methods can help reduce anxiety and stress levels.
- Professional Help: Consult a mental health professional for personalized treatment plans, including therapy and medication if necessary. A comprehensive approach is often most effective in managing skin-picking disorders.
Stopping dermatillomania requires self-awareness and active efforts to identify triggers, modify behaviors, and regulate emotions. Seeking professional help is also important for long-term management. With perseverance and a comprehensive approach, overcoming this disorder and having healthier skin is possible.
How to Manage Dermatillomania in the Long Term?
Managing long-term dermatillomania, or skin-picking disorder, requires psychotherapy, medication, and a structured routine, according to Ravipati P et al.’s 2021 study “Strategies for Developing Protective Biomaterials/Cloth. Pharmaceutics” published in the Pharmaceutical Journal. Psychotherapy, especially cognitive behavioral therapy (CBT), is foundational in helping individuals identify triggers and develop healthier coping strategies.
This therapy often includes habit reversal training, which teaches patients to replace skin picking with alternative behaviors, such as squeezing a stress ball or engaging in other tactile activities. Additionally, medications like selective serotonin reuptake inhibitors (SSRIs) can help manage underlying anxiety and compulsive behaviors.
Regular follow-ups with psychiatrists ensure that individuals receive tailored support and adjustments to their treatment as needed, fostering a sense of accountability and community. Incorporating self-care practices is equally critical in the long-term management of dermatillomania.
Individuals are encouraged to maintain a structured routine that includes mindfulness techniques, such as meditation or deep breathing exercises, to reduce stress and anxiety that may trigger skin-picking episodes. Creating a supportive environment, such as informing friends and family about the condition, enhances accountability and provides emotional support.
How Excoriation Disorder Impacts Quality of Life?
Excoriation disorder impacts quality of life, causing physical impacts, social and emotional toil, social withdrawal and anxiety, low self-esteem, and impact on daily functioning, according to Ekore RI et al.’s study, “Excoriation (skin-picking) Disorder Among Adolescents and Young Adults With Acne-induced Postinflammatory Hyperpigmentation and Scars” published in the International Journal of Dermatology.
- Physical Impacts: Excoriation disorder leads to significant physical health issues, including infections and permanent scarring. The repetitive skin picking often results in open wounds, which become infected and require surgical interventions like skin grafts to repair the damage. The physical consequences are severe, leading to chronic pain and discomfort and the potential for long-term skin deformities.
- Social and Emotional Toll: Individuals with excoriation disorder frequently experience heightened levels of anxiety and shame associated with their condition. The visible effects of skin picking lead to embarrassment, contributing to a diminished quality of life. Individuals feel compelled to hide their skin, leading to further emotional distress and isolation from social interactions.
- Social Withdrawal and Anxiety: The disorder often results in social withdrawal as individuals avoid situations where their skin might be exposed. This withdrawal increases feelings of loneliness and anxiety, creating a cycle that further entrenches the disorder. The fear of judgment or negative perception from others leads to avoidance of social engagements, impacting relationships and overall social functioning.
- Low Self-Esteem and Body Image Issues: Excoriation disorder significantly affects self-esteem and body image. Individuals may develop negative perceptions of themselves due to the visible damage caused by their skin picking. This leads to feelings of worthlessness or inadequacy, further compounding emotional difficulties and mental health issues such as depression.
- Impact on Daily Functioning and Productivity: Skin picking’s compulsive nature interferes with daily activities, including work or school performance. Individuals may find it difficult to concentrate or engage fully in tasks due to preoccupation with their skin-picking behavior or the resulting physical discomfort. This impairment leads to decreased productivity and challenges in maintaining employment or academic success.
Excoriation disorder impacts an individual’s overall life and well-being. It is important to seek professional help for proper diagnosis and treatment to improve symptoms and manage the disorder’s emotional and physical effects.
Can Dermatillomania Cause Cancer?
No. Dermatillomania cannot cause cancer as there is no direct evidence linking it to the development of skin cancer. According to Wunderlich K et al.’s 2024 study, “Risk Factors and Innovations in Risk Assessment for Melanoma, in the Cancer’s Journal, the primary risk factors for skin cancer are related to UV exposure and genetic predispositions rather than habits like skin-picking.
The misconception that dermatillomania directly causes skin cancer may stem from its association with chronic wounds. These wounds can become infected, leading to complications that indirectly increase health risks. However, the consensus remains that frequent skin picking does not inherently elevate the risk of developing skin cancer. Instead, maintaining good skin hygiene and seeking treatment for dermatillomania can mitigate potential complications associated with this behavior.
Can You Die from Dermatillomania?
Yes, severe dermatillomania can lead to life-threatening health risks, primarily through the complications arising from repeated skin picking, according to Kim DI, Garrison RC, et al.’s 2013 post “A Near Fatal Case of Pathological Skin Picking” published in the American Journal of Case Reports. While the condition itself is not fatal, the consequences of excessive skin picking can be dangerous and potentially deadly.
Skin picking repeatedly damages the skin’s protective barrier, making it vulnerable to infections. With continued picking, bacteria from hands and nails easily infect open wounds and cause serious skin infections. In severe cases, these infections spread to other body parts or enter the bloodstream, leading to sepsis. Sepsis is a life-threatening condition that can quickly progress if left untreated.
Is Dermatillomania a Disability?
Yes. Dermatillomania is considered a disability as it falls under the category of Obsessive-Compulsive and Related Disorders in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), according to Regier DA et al.’s 2013 post “The DSM-5: Classification and criteria changes” published in the World Psychiatry Journal.
The Americans with Disabilities Act (ADA) also considers dermatillomania a disability. This law prohibits discrimination against individuals with disabilities in all areas of public life, including education, employment, transportation, and access to goods and services. Individuals with dermatillomania are protected under this law and have the right to reasonable accommodations in the workplace and other settings.
To qualify as a disability under legal definitions, particularly for Social Security Disability Insurance (SSDI), individuals must demonstrate that their condition causes substantial limitations in their ability to perform work-related activities over a continuous period of at least 12 months.
Contact us today to schedule an initial assessment or to learn more about our services. Whether you are seeking intensive outpatient care or simply need guidance on your mental health journey, we are here to help.
How to Help Someone with Skin-Picking Disorder?
To help someone with skin-picking disorder, offer unconditional support, educate yourself, encourage professional help, identify triggers together, and promote healthy alternatives, according to Jafferany M et al. ‘s 2019 review, “Skin-Picking Disorder: A Guide to Diagnosis and Management,” published in the CNS Drugs Journal.
- Offer Unconditional Support: Let your loved one know you are there for them without judgment. This can help reduce feelings of shame and embarrassment associated with dermatillomania.
- Educate Yourself: Learn about dermatillomania to understand what your loved one is experiencing. This knowledge can help you provide informed support and reduce stigma.
- Encourage Professional Help: Suggest seeking therapy or counseling. Offer to accompany them to appointments, which may make them feel more comfortable.
- Identify Triggers Together: Help your loved one recognize situations or emotions that lead to skin picking. Keeping a trigger diary can be a helpful tool.
- Promote Healthy Alternatives: Encourage alternative coping strategies, such as using fidget toys, engaging in hobbies, or practicing mindfulness to manage urges.
Remember, it takes time and patience to recover from a skin-picking disorder. Be a source of support and understanding for your loved one as they navigate their journey towards healing. Keep open communication and educate yourself on supporting them in their recovery process. With your help, they can overcome this challenging disorder.
Share This Post

TREATMENTS WE OFFER
Are you covered for treatment?









LAOP is an approved provider for Blue Shield of California and Magellan, while also accepting many other major insurance carriers.
Check Coverage Now!

