What Is PTSD in Veterans? Causes, Symptoms, and Proven Treatments

Post-traumatic stress disorder (PTSD) in veterans is a clinically recognized mental health condition triggered by direct exposure to, or witnessing of, actual or threatened death, serious injury, or sexual violence during military service. PTSD causes lasting changes in how the brain and body respond to stress, memory, and perceived threat — producing intrusive memories of trauma, avoidance of trauma-related cues, negative changes in thinking and mood, and hyperarousal (a state of heightened physiological alertness) that persist for more than one month and impair daily functioning. It is a treatable medical condition, not a character flaw or sign of weakness.
Veterans develop PTSD at significantly higher rates than the general population. Post-9/11 combat veterans have 4.87 times the probability of a PTSD diagnosis compared to civilians — and among those who served in the heaviest combat roles, rates reach 29% lifetime prevalence (Ortiz Diaz et al., 2024; nchstats.com, 2025). Despite this burden, stigma embedded in military culture remains a documented barrier to care: many veterans avoid treatment out of concern about appearing weak or that disclosure will harm their careers. The consequences of untreated PTSD are severe — veterans with PTSD die by suicide at a rate of 51.3 per 100,000 person-years, nearly four times the general adult population rate of 13.2 (Forehand et al., 2022; Mission Roll Call, 2025).
Highlights
▸ 17.6 veterans die by suicide every day — an average drawn from 6,407 veteran suicides recorded in 2022, per the VA’s 2024 National Veteran Suicide Prevention Annual Report.
▸ Post-9/11 combat veterans have 4.87 times the probability of PTSD diagnosis compared to civilians, with lifetime prevalence reaching 29% among OIF/OEF (Operation Iraqi Freedom/Enduring Freedom) veterans (Ortiz Diaz et al., 2024).
▸ Veterans with PTSD face a suicide rate of 51.3 per 100,000 — nearly four times the general population rate — making PTSD diagnosis one of the most significant suicide risk factors in the veteran population (Mission Roll Call, 2025).
▸ Female veterans are disproportionately affected: women veterans have a 13% lifetime PTSD prevalence (vs. 6–7% for male veterans), and female veteran suicide rates are 92% higher than those of civilian women (Mission Roll Call, 2025).
▸ The 2023 VA/DoD Clinical Practice Guideline — the most recent update — identifies three trauma-focused psychotherapies as first-line treatments: Cognitive Processing Therapy (CPT), Prolonged Exposure (PE), and EMDR (Schnurr et al., 2024).
▸ Intensive outpatient PTSD treatment (IOP) achieves completion rates of 87.3% compared to 46.2% for weekly treatment, with equivalent large treatment effect sizes — a critical finding for addressing the veteran dropout problem (Yamokoski et al., 2023 via PTSD Research Quarterly, 2024).
▸ The VA’s 2025 federal budget allocates $17 billion for mental health services and $583 million specifically for suicide prevention outreach — more than eight times the VA’s 2001 total budget (Mission Roll Call, 2025).
Did you know most health insurance plans cover mental health treatment? Check your coverage online now.
What Is PTSD in Veterans?
PTSD in veterans is a trauma- and stress-related psychiatric disorder that develops after exposure to traumatic events inherent to military service — including combat, military sexual trauma (MST), witnessing casualties, or situations involving moral injury (distress caused when actions violate a person’s core moral beliefs). Unlike the general civilian population, veterans often experience multiple traumatic events across prolonged deployments, which compounds both the risk of developing PTSD and the complexity of treating it.
The DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) defines PTSD across four symptom clusters, each of which must be present for at least one month and cause significant functional impairment: intrusion symptoms (such as flashbacks and nightmares), avoidance of trauma-related stimuli, negative alterations in cognition and mood, and marked alterations in arousal and reactivity (hyperarousal). Veterans may also experience dissociative symptoms — a subtype added in the DSM-5 — which include depersonalization (feeling detached from oneself) and derealization (feeling that the world is unreal).
PTSD is fundamentally different from the normal psychological stress that all military personnel experience. Combat stress — characterized by temporary anxiety, heightened alertness, and sleep disruption during deployment — typically resolves when the stressor is removed. PTSD is distinguished by the persistence of these symptoms beyond the acute stress period, the development of intrusive re-experiencing of trauma, and the progressive functional impairment that occurs when symptoms are left untreated. The transition from acute stress reaction to PTSD reflects underlying neurobiological changes in the amygdala (the brain’s threat-detection center), hippocampus (involved in memory consolidation), and prefrontal cortex (which regulates emotional responses and decision-making) that make the trauma response chronic rather than self-resolving.
What Causes PTSD in Veterans?
The causes of PTSD in veterans are rooted in the types, severity, and duration of trauma encountered during military service — combined with biological vulnerability factors, deployment conditions, and the adequacy of post-deployment support. Unlike PTSD in civilians, which more commonly follows a single traumatic event, veteran PTSD typically emerges from prolonged or repeated exposure to multiple stressors.
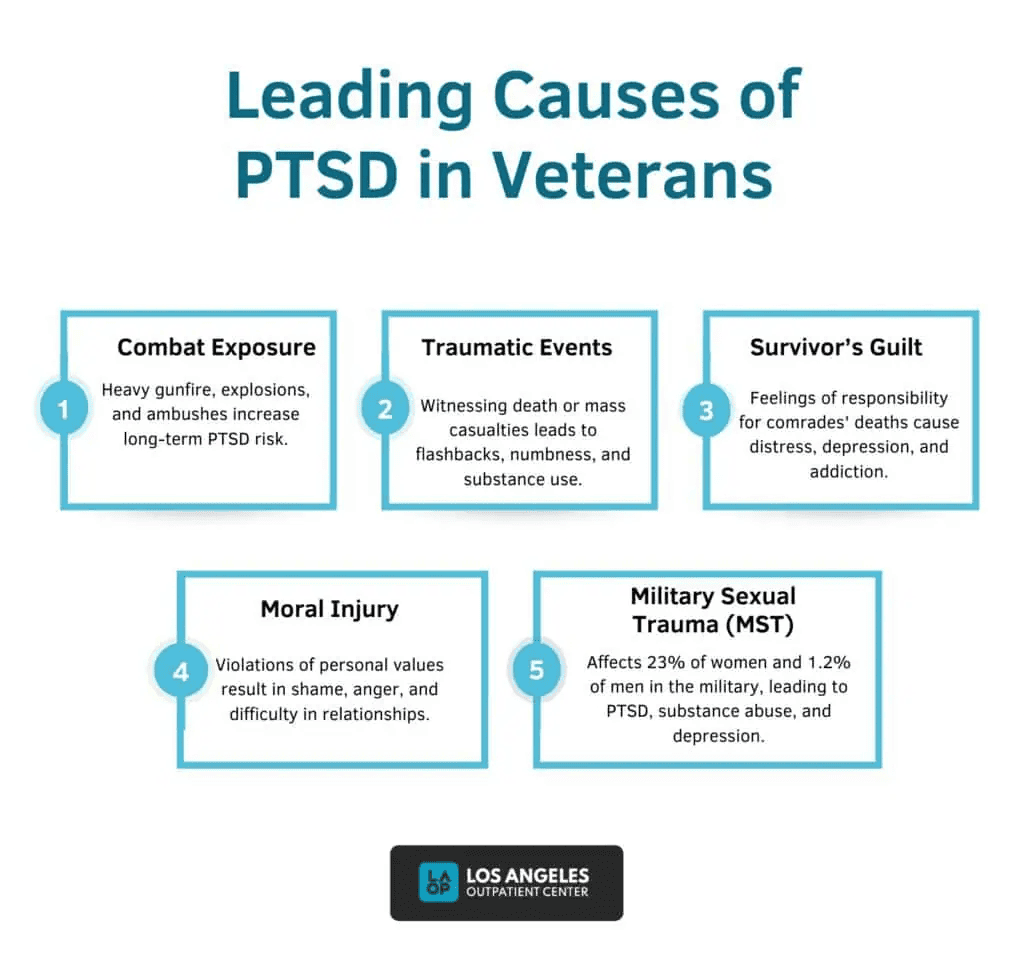
Combat Exposure
Combat exposure is the most frequently studied cause of PTSD in veterans. Experiences such as direct firefights, improvised explosive device (IED) detonations, witnessing the death or severe injury of fellow service members, and proximity to mass casualties produce intense, involuntary trauma memories that form the neurobiological substrate of PTSD. Veterans of high-intensity combat theaters — particularly Army and Marine Corps infantry — have higher PTSD rates than those in support roles, reflecting a dose-response relationship between combat exposure and PTSD risk.
Military Sexual Trauma (MST)
Military sexual trauma (MST) — defined by the VA as sexual harassment or assault experienced during military service — is a significant and disproportionately underacknowledged cause of PTSD in veterans. Current VA screening data show that approximately 1 in 3 women veterans and 1 in 50 male veterans report MST when screened, and MST-related trauma is strongly associated with PTSD, depression, and substance use disorders (nchstats.com, 2025). Women veterans using VA healthcare services have an approximately 13% lifetime PTSD prevalence — more than double the rate of male veterans — in significant part because of MST exposure. MST-related PTSD often differs from combat-related PTSD in its presentation: shame, self-blame, interpersonal trust difficulties, and reluctance to seek care within the same institutional structure in which the trauma occurred are common.
Moral Injury
Moral injury is a construct distinct from PTSD, but which frequently co-occurs with it in the veteran population. Moral injury refers to the deep psychological distress that results from perpetrating, witnessing, or failing to prevent actions that violate a person’s moral beliefs — or from feeling betrayed by leaders or institutions. In military contexts, this may include following orders that result in civilian casualties, perceived failures to protect fellow service members, or institutional experiences of injustice. Research by RAND’s 2025 analysis of veteran suicide highlighted that veterans with moral injury show higher rates of suicide, likely mediated by shame, guilt, and a damaged sense of self-worth (RAND, 2025). Most standard PTSD treatments address traumatic memories; clinicians working with veterans should additionally assess for and address moral injury, which may require specific therapeutic approaches such as Adaptive Disclosure therapy or meaning-based interventions.
Contact us today to schedule an initial assessment or to learn more about our services. Whether you are seeking intensive outpatient care or simply need guidance on your mental health journey, we are here to help.
Traumatic Brain Injury (TBI)
Traumatic brain injury (TBI) — particularly mild TBI from blast exposure, a signature injury of the Iraq and Afghanistan conflicts — frequently co-occurs with PTSD and shares overlapping symptoms including memory problems, concentration difficulties, irritability, headaches, and sleep disturbance. The co-occurrence of TBI and PTSD complicates both diagnosis (because symptoms are difficult to attribute to one condition versus the other) and treatment (because standard exposure-based PTSD therapies may need modification for patients with significant cognitive impairment). Approximately 12–22% of post-9/11 veterans are estimated to have co-occurring TBI and PTSD (LAOP original article; VA data).
Risk and Protective Factors
Vulnerability to developing PTSD after trauma is not uniform. Key risk factors include:
- Pre-existing mental health conditions: Prior anxiety, depression, or trauma history increases PTSD susceptibility.
- Multiple deployments: Repeated exposure without adequate recovery time between deployments compounds cumulative stress load.
- Lack of post-deployment social support: Weak social support networks are among the most consistently identified risk factors for PTSD across the research literature.
- Childhood adversity: Adverse childhood experiences (ACEs) increase biological stress reactivity and PTSD vulnerability in adulthood.
- LGBTQ+ identity: LGBTQ+ veterans experience rates of suicide up to seven times higher than non-LGBTQ+ veterans — reflecting the compounding effect of minority stress on top of military trauma (Stop Soldier Suicide, 2025).
Key protective factors that reduce PTSD risk include strong unit cohesion during deployment, access to mental health care during and after service, perceived institutional support, and strong post-discharge social and family networks.
What Are the Types of PTSD That Affect Veterans?

The types of PTSD affecting veterans include acute PTSD, chronic PTSD, complex PTSD, delayed-onset PTSD, and the dissociative subtype — each with distinct onset patterns, symptom profiles, and treatment implications. Understanding the type and chronicity of PTSD guides clinical decision-making about the level of care and treatment format.
Acute PTSD
Acute PTSD is defined as PTSD with a symptom duration of one to three months following trauma. Early intervention during this window — including trauma-focused psychotherapy — can prevent the consolidation of acute stress reactions into chronic PTSD. Without intervention, a significant proportion of veterans with acute PTSD transition to chronic presentations.
Chronic PTSD
Chronic PTSD is defined as PTSD with symptoms lasting more than three months and is the most common presentation in treatment-seeking veterans. Chronic PTSD is characterized by deeply ingrained avoidance patterns, more pronounced negative alterations in mood and cognition, and higher rates of co-occurring depression, substance use, and physical health conditions. A 50-year longitudinal study of Vietnam veterans found that 9% continued to meet full PTSD diagnostic criteria five decades after deployment, and 25% had sub-threshold PTSD symptoms persisting long-term — underscoring that chronic PTSD does not simply resolve on its own without treatment (Stellman et al., 2025).
Are you covered for treatment?
LAOP is an approved provider for Blue Shield of California and Magellan, while also accepting many other major insurance carriers.
Check Coverage Now!Complex PTSD
Complex PTSD (C-PTSD) results from prolonged, repeated trauma exposure — such as captivity, extended imprisonment, or sustained abuse during service — rather than from discrete traumatic events. C-PTSD includes the standard PTSD symptom clusters plus three additional domains of disturbance: emotional dysregulation (difficulty managing intense emotions), negative self-concept (chronic feelings of shame, guilt, and worthlessness), and relational disturbances (difficulty forming or maintaining close relationships). Research on UK armed forces veterans found that 65.7% of those with complex PTSD had severe difficulty with emotion regulation, and scored 12.4% lower on executive function tasks — directly affecting their ability to work, plan, and maintain relationships (Biscoe et al., 2024). Treatment of C-PTSD typically requires longer-term, phase-based approaches and may need to address emotion regulation and relational skills before direct trauma processing.
Delayed-Onset PTSD
Delayed-onset PTSD is diagnosed when the full syndrome does not emerge until at least six months after the traumatic event — sometimes years or even decades later. This presentation is particularly important for older veterans of earlier conflicts (Vietnam, Gulf War) who may present with new or worsening PTSD symptoms in later life, sometimes triggered by retirement, physical health changes, or bereavement that removes the routines and distractions that had previously contained symptoms.
PTSD with Dissociative Subtype
The dissociative subtype of PTSD — added in the DSM-5 — is characterized by prominent depersonalization and derealization alongside standard PTSD symptoms. This subtype is associated with higher rates of childhood trauma, greater overall symptom severity, and may require modified treatment approaches because standard exposure-based therapies can paradoxically increase dissociative symptoms if applied without adequate stabilization.
What Are the Symptoms of PTSD in Veterans?
The symptoms of PTSD in veterans fall into four DSM-5 clusters, each of which must be present and cause significant distress or functional impairment for a diagnosis to be made.
Cluster 1: Intrusion Symptoms
- Flashbacks: Involuntary, vivid re-experiencing of the traumatic event as if it were happening in the present moment — triggered by sensory cues such as sounds, smells, or visual stimuli that resemble the original trauma. Among veterans with PTSD, nightmare prevalence is as high as 72%, severely impairing sleep quality (Worley et al., 2024).
- Nightmares: Recurring, distressing dreams directly related to the traumatic event, causing sleep disruption and daytime fatigue.
- Intrusive memories: Unwanted, distressing memories of trauma that interrupt concentration and daily activities.
- Psychological distress at trauma cues: Intense emotional reactions triggered by reminders of the trauma.
- Physiological reactivity to cues: Physical responses — sweating, heart pounding, trembling — triggered by trauma-related stimuli.
Rediscover Life at Los Angeles Outpatient Center
Get the compassionate mental health support you deserve. We're here to help you reclaim joy, wellness, and a brighter future.
Our Facility
Cluster 2: Avoidance
- Avoidance of trauma-related thoughts or feelings: Active efforts to suppress or push away memories, feelings, or thoughts associated with the trauma.
- Avoidance of external reminders: Avoiding people, places, activities, objects, or situations that trigger trauma memories — including crowded spaces, fireworks, backfiring vehicles, or even news coverage of military operations.
Cluster 3: Negative Alterations in Cognition and Mood
- Inability to recall important aspects of the trauma: Dissociative amnesia specifically related to the traumatic event.
- Persistent negative beliefs: Distorted beliefs about oneself, others, or the world — such as ‘I am permanently damaged,’ ‘No one can be trusted,’ or ‘The world is completely dangerous.’
- Persistent negative emotional states: Chronic fear, horror, anger, guilt, or shame.
- Emotional numbing: Markedly diminished interest or participation in activities; feeling detached from others; restricted positive emotional range.
- Feelings of estrangement: Sense of being cut off from other people; inability to connect with family or friends despite genuine relationships.
Cluster 4: Hyperarousal and Reactivity
- Hypervigilance: Persistent state of heightened alertness — continuously scanning for threat even in safe environments.
- Exaggerated startle response: Extreme reaction to unexpected sounds or movements, including sudden sounds that resemble gunfire.
- Irritability and angry outbursts: Often with little provocation; may manifest as verbal or physical aggression, causing relationship and legal problems.
- Difficulty concentrating: Cognitive impairment affecting work performance, decision-making, and daily task completion.
- Sleep disturbance: Difficulty falling or staying asleep, or non-restorative sleep — the most commonly reported PTSD symptom in veteran populations.
- Reckless or self-destructive behavior: Including substance use, risky driving, and other behaviors that reflect a changed relationship to personal safety.
How Does PTSD Affect Veterans’ Lives?
The effects of PTSD on veterans’ lives extend well beyond psychiatric symptoms — producing measurable, documented harm across physical health, occupational functioning, relationships, housing stability, and mortality. These effects are interconnected: untreated PTSD drives substance use, which worsens financial instability, which increases isolation, which elevates suicide risk.
- Suicide: PTSD is one of the most significant risk factors for veteran suicide. Veterans with PTSD die by suicide at a rate of 51.3 per 100,000 person-years — compared to 13.2 in the general adult population (Forehand et al., 2022). In 2022, 17.6 veterans died by suicide every day (VA, 2024). Among veterans who died by suicide with a mental health diagnosis, 40% had PTSD (RAND, 2025). However, it is critical to note that the presence of comorbid conditions — particularly depression and substance use disorder — significantly amplifies suicide risk beyond PTSD alone. Moral injury and firearms access are identified as additional key factors.
- Substance use: Alcohol and drug use disorders frequently develop as veterans attempt to self-medicate PTSD symptoms — numbing hyperarousal with alcohol, managing insomnia with opioids, or reducing social anxiety with sedatives. Nearly 50% of veterans with PTSD develop a co-occurring substance use disorder (Seal et al., 2011). Sedative use disorder carries the highest suicide rate of any substance in the veteran population — 236.7 per 100,000 (RAND, 2025).
- Physical health consequences: PTSD drives chronic physiological stress that damages cardiovascular, immune, and metabolic systems. A 50-year follow-up study of Vietnam veterans found that 28% of those with PTSD had been diagnosed with heart disease and 46.5% with arthritis — significantly higher rates than veterans without PTSD (Stellman et al., 2025). Veterans with PTSD have a 50% greater risk of heart failure over seven years compared to those without PTSD.
- Relationship and family impact: Up to 70% of veterans with PTSD report relationship distress, compared to 30% without PTSD. PTSD-driven emotional numbing, irritability, and avoidance of intimacy erode marriages, partnerships, and parenting relationships. Secondary traumatization — where family members develop trauma-related symptoms from exposure to the veteran’s PTSD — is documented and frequently overlooked.
- Occupational and financial consequences: Approximately 25% of veterans with PTSD are unemployed, compared to 8% of veterans without PTSD. Workplace difficulties include conflict with authority, concentration problems, hypervigilance, and difficulty tolerating crowded or loud environments. Financial instability compounds mental health vulnerability in a feedback cycle.
- Homelessness: PTSD is strongly associated with veteran homelessness — which decreased by 7% between 2023 and 2024, reflecting recent VA investment, though the underlying mental health drivers remain significant (Mission Roll Call, 2025). Veterans experiencing homelessness frequently have co-occurring PTSD and substance use disorders, requiring integrated housing-plus-treatment approaches.
How Is PTSD in Veterans Diagnosed?
PTSD in veterans is diagnosed using DSM-5 criteria evaluated through structured clinical interviews and validated screening instruments. Correct diagnosis is essential: a 2024 study found that veterans unaware of their PTSD diagnosis face significantly worse mental health outcomes — including higher rates of depression, anxiety, and overall poorer functioning — compared to those who understand their diagnosis (Holder et al., 2024).
The primary screening and diagnostic tools used in veteran settings include:
- PC-PTSD-5 (Primary Care PTSD Screen for DSM-5): A 5-item screen recommended by the 2023 VA/DoD Clinical Practice Guideline as the initial assessment tool. Identifies probable PTSD and determines whether further evaluation is needed.
- PCL-5 (PTSD Checklist for DSM-5): A 20-item self-report measure assessing all four DSM-5 PTSD symptom clusters. Scores above 31–33 indicate clinically significant PTSD. Also used to track symptom change during treatment.
- CAPS-5 (Clinician-Administered PTSD Scale for DSM-5): The gold-standard structured diagnostic interview for PTSD, administered by a trained clinician. Provides both a diagnosis and a severity rating.
- Comprehensive comorbidity assessment: Given the high co-occurrence of depression, substance use, TBI, and other anxiety disorders in the veteran population, thorough assessment of co-occurring conditions is clinically essential and directly affects treatment planning.
The 2023 VA/DoD CPG (Clinical Practice Guideline) recommends that PTSD screening be incorporated into routine VA primary care visits for all veterans, with the PC-PTSD-5 as the initial tool. Positive screens require follow-up clinical evaluation before a diagnosis is made.
Did you know most health insurance plans cover mental health treatment? Check your coverage online now.
What Are the Evidence-Based Treatments for PTSD in Veterans?
Evidence-based treatments for PTSD in veterans are specific psychotherapeutic and pharmacological interventions validated in randomized controlled trials to reduce PTSD symptom severity, improve functioning, and decrease suicide risk. The 2023 VA/DoD Clinical Practice Guideline — the most authoritative and current clinical standard in the United States — provides the following hierarchy of recommendations.
| Treatment | VA/DoD 2023 CPG Rating | Typical Format | Key Mechanism |
|---|---|---|---|
| Cognitive Processing Therapy (CPT) | Strong recommendation — first-line | 12 sessions, individual or group | Challenges stuck points about trauma, safety, trust, power, esteem, and intimacy |
| Prolonged Exposure (PE) | Strong recommendation — first-line | 8–15 sessions, individual | Imaginal and in-vivo exposure; emotional processing of trauma memory |
| EMDR | Strong recommendation — first-line | 6–12+ sessions; more for combat trauma | Bilateral stimulation while recalling trauma; reduces emotional charge of memories |
| Written Exposure Therapy (WET) | Suggested (2023 addition) | 5 sessions — shortest format | Structured trauma narrative writing; lower burden; comparable efficacy to PE |
| MBSR | Suggested | 8-week group program | Mindfulness-based stress reduction; reduces hyperarousal; improves emotional regulation |
| Prazosin | Suggested (for nightmares) | Daily medication | Alpha-1 blocker; reduces nightmare frequency and severity |
Cognitive Processing Therapy (CPT)
CPT is one of the most extensively researched and widely disseminated evidence-based treatments for PTSD in veterans. CPT focuses on identifying and modifying stuck points (unhelpful beliefs about the trauma and its meaning) in five thematic domains: safety, trust, power/control, esteem, and intimacy. In a landmark RCT of 916 veterans randomized to CPT or Prolonged Exposure, PTSD symptoms improved significantly in both treatments, with CPT showing somewhat faster improvements in depression outcomes (VA National Center for PTSD, 2025).
An important 2024 finding is the evidence for intensive/massed CPT formats — where sessions are delivered daily over 1–4 weeks rather than weekly across 12 weeks. Studies show that intensive outpatient PTSD treatment (IOP) achieves completion rates of 87.3% compared to 46.2% for weekly treatment, with equivalent large effect sizes. This is clinically significant because treatment dropout is one of the primary reasons standard-format CPT fails to reach its full potential in veteran populations (PTSD Research Quarterly, 2024). Intensive formats are increasingly available at VA specialized PTSD programs.
Prolonged Exposure (PE)
PE is based on emotional processing theory and involves two complementary exposure components: imaginal exposure (repeatedly recounting the trauma memory in detail) and in-vivo exposure (gradually confronting avoided trauma-related situations in real life). PE works by activating the trauma memory and providing the conditions necessary for new learning to occur — allowing the brain to update its threat model and reduce the emotional charge of traumatic memories. A 2024 state-of-the-science review confirmed PE’s strong efficacy profile across veteran and military populations, with female veterans completing PE being 1.8 times more likely to no longer meet PTSD diagnostic criteria at follow-up compared to control conditions (McLean & Foa, 2024).
EMDR (Eye Movement Desensitization and Reprocessing)
EMDR involves the veteran recalling trauma memories while simultaneously engaging in bilateral sensory stimulation — most commonly guided eye movements. The 2023 VA/DoD CPG rates EMDR as a strong recommendation for PTSD treatment, though it notes a smaller evidence base in veteran populations specifically compared to civilian samples and fewer studies in active-duty service members. EMDR has particular utility for combat trauma with multiple traumatic events requiring 12 or more sessions, and for PTSD with comorbid moral injury presentations (PMC, 2016). Both daily intensive and weekly EMDR formats have been validated, with intensive formats reducing treatment time without compromising outcomes.
Written Exposure Therapy (WET)
Written Exposure Therapy (WET) is a newer evidence-based approach added to VA/DoD CPG recommendations in 2023. WET involves five structured sessions in which the veteran writes about their trauma experience according to specific guidelines designed to facilitate emotional processing. WET has demonstrated non-inferiority to PE in at least one large RCT, produces large symptom reductions through 3-month follow-up in open trials, and requires significantly fewer sessions than CPT or PE — making it an important option for veterans with access barriers, high treatment burden, or initial reluctance toward more intensive approaches (PTSD Research Quarterly, 2024).
Contact us today to schedule an initial assessment or to learn more about our services. Whether you are seeking intensive outpatient care or simply need guidance on your mental health journey, we are here to help.
Pharmacotherapy
The 2023 VA/DoD CPG recommends individual trauma-focused psychotherapy (CPT, PE, EMDR) over medication as the primary treatment for PTSD in veterans. This represents an important update from prior guidance, reflecting evidence that medications produce smaller and less durable effects on core PTSD symptoms than trauma-focused psychotherapy. However, pharmacotherapy plays an important adjunctive role:
- SSRIs/SNRIs: Sertraline and paroxetine are FDA-approved for PTSD; venlafaxine is also supported. These address depression and anxiety symptoms that frequently co-occur with PTSD.
- Prazosin: An alpha-1 blocker suggested in the CPG specifically for PTSD-related nightmares — particularly useful when sleep disturbance is prominent and impairing.
- Medications to avoid: The 2023 CPG explicitly recommends against benzodiazepines (a class of sedatives) for PTSD, as they are associated with dependency and do not address core trauma symptoms — and sedative use disorder carries the highest suicide rate of any substance in the veteran population.
Adjunctive and Emerging Approaches
Several approaches have emerging evidence or are used adjunctively alongside first-line treatments:
- Mindfulness-Based Stress Reduction (MBSR): Suggested in the 2023 CPG as an adjunctive option; supported by evidence for reducing hyperarousal and improving emotional regulation in veterans.
- Psychiatric service dogs: A 2024 systematic review and meta-analysis found that psychiatric assistance dogs produce clinically significant reductions in PTSD severity in veterans — with service dogs trained to interrupt panic attacks, wake veterans from nightmares, and provide social grounding in public spaces (Leighton et al., 2024).
- VA Telehealth: Remote delivery of CPT, PE, and EMDR through VA Video Connect has demonstrated equivalent outcomes to in-person delivery, significantly expanding access for veterans in rural areas or those with mobility or transportation barriers.
How Does PTSD in Veterans Differ From PTSD in Civilians?
PTSD in veterans differs from PTSD in civilians in the nature and duration of trauma exposure, the types of symptoms that predominate, the co-occurring conditions that complicate treatment, and the specific barriers to care. The most precise quantification of this difference comes from a 2024 analysis: post-9/11 combat veterans have 4.87 times the probability of a PTSD diagnosis compared to civilian counterparts (Ortiz Diaz et al., 2024).
| Factor | PTSD in Veterans | PTSD in Civilians |
|---|---|---|
| Primary trauma types | Combat, MST, moral injury, prolonged operational stress | Accidents, assaults, natural disasters, interpersonal violence |
| Trauma duration | Often prolonged and repetitive across multiple deployments | More commonly single-incident trauma |
| Unique features | Moral injury, survivor guilt, TBI comorbidity, military culture stigma | Less likely to involve moral injury or stigma-related barriers |
| Suicide rate | 33.9/100,000 (unadjusted, 2021); 51.3/100,000 with PTSD diagnosis | ~16.7/100,000 general adult population |
| Treatment barriers | Stigma, perceived career impact, isolation from civilian culture, VA access gaps | Stigma, cost, and geographic access — but fewer military-specific barriers |
| Post-9/11 probability | 4.87x higher probability of PTSD vs civilians (Ortiz Diaz et al., 2024) | Baseline reference population |
What Barriers Prevent Veterans From Seeking PTSD Treatment?
Barriers to PTSD treatment are among the most clinically significant factors in veteran mental health outcomes — because they translate into delayed diagnosis, chronic deterioration, and elevated suicide risk. A 2024 study found that veterans unaware of their PTSD diagnosis had substantially worse mental health outcomes than those who received and understood their diagnosis, directly linking diagnostic awareness to prognosis (Holder et al., 2024).
- Stigma and military culture: Military culture traditionally valorizes self-reliance, stoicism, and toughness — directly conflicting with help-seeking behavior. Veterans frequently report concerns about being perceived as weak by peers, or that disclosing PTSD will harm their career prospects during or after service.
- Perceived lack of need or minimization: Many veterans minimize their symptoms, attribute them to normal post-service adjustment, or believe they should be able to manage without help — particularly those with delayed-onset PTSD or incomplete insight into the full symptom picture.
- Practical access barriers: Geographic distance from VA facilities, long wait times, lack of PTSD-specialized providers in community settings, and transportation challenges — particularly for veterans in rural areas — create structural barriers that impede even motivated veterans from accessing timely care.
- Treatment dropout: Among veterans who do engage with treatment, dropout from evidence-based therapies is a significant problem, with weekly CPT and PE completing at rates of only 46% in some studies. Intensive formats (IOP) dramatically improve completion to 87%, suggesting that the format — not the content — of treatment contributes substantially to dropout (PTSD Research Quarterly, 2024).
- Concerns about medication: Some veterans resist treatment because they fear medication side effects, dependency, or emotional blunting. Clear clinician communication about the 2023 CPG’s preference for psychotherapy-first — with medication as adjunct rather than primary treatment — can reduce this barrier.
How Can Family Members Support a Veteran With PTSD?
Supporting a veteran with PTSD requires understanding that the symptoms — including emotional withdrawal, irritability, hypervigilance, and avoidance — are neurobiological consequences of trauma, not personal choices or character flaws. Family members who lack this understanding commonly report feeling rejected, confused, or targeted by behaviors that are actually symptoms of an untreated medical condition.
- Learn about PTSD as a medical condition: Understanding that hypervigilance, startle responses, and emotional numbing are driven by neurobiological changes following trauma — rather than personal hostility or disinterest — reduces family conflict and increases therapeutic patience.
- Avoid avoidance accommodation: Well-meaning family members sometimes participate in or enable avoidance behaviors — declining to go to crowded places, avoiding certain topics, or insulating the veteran from triggering situations. While this reduces short-term distress, it reinforces avoidance long-term and impedes recovery.
- Do not minimize: Statements like ‘just get over it’ or ‘everyone who served has been through this’ invalidate the veteran’s experience and are known barriers to treatment engagement.
- Address crises directly: Increased withdrawal, escalating substance use, giving away possessions, or statements about not wanting to live require direct action — not indirect engagement. Contact the Veterans Crisis Line (988, then press 1) or take the veteran to an emergency room if safety is at immediate risk.
- Seek your own support: Secondary traumatization — the development of trauma-related symptoms in family members of PTSD sufferers — is a documented and underdiagnosed condition. Family members benefit significantly from individual therapy, NAMI’s Family-to-Family education, and VA Caregiver Support Programs.
Are you covered for treatment?
LAOP is an approved provider for Blue Shield of California and Magellan, while also accepting many other major insurance carriers.
Check Coverage Now!When Should a Veteran Seek Help for PTSD?
A veteran should seek help for PTSD when trauma-related symptoms are causing significant distress, impairing functioning at work or in relationships, or producing behaviors — including substance use, self-isolation, or reckless conduct — that signal deteriorating mental health. There is no symptom severity threshold that must be met before seeking evaluation. Earlier engagement with care consistently predicts better outcomes.
Seek urgent care immediately when:
- The veteran expresses thoughts of suicide, self-harm, or hopelessness about the future — contact the Veterans Crisis Line immediately: call 988 and press 1, text 838255, or chat online at VeteransCrisisLine.net.
- There is escalating substance use (particularly alcohol, opioids, or sedatives) — this combination dramatically elevates suicide risk.
- The veteran becomes socially isolated to the point of not leaving the home, losing employment, or severing all family contact.
- Physical health emergencies such as chest pain, cardiovascular symptoms, or severe sleep deprivation occur — PTSD accelerates cardiovascular risk and may require immediate medical attention.
For non-urgent situations, initial points of contact include:
- VA primary care or mental health services: Veterans enrolled in VA healthcare can access PTSD evaluation through their VA primary care provider or directly at VA mental health clinics.
- Vet Centers: Community-based VA outreach facilities offering free counseling, group therapy, and peer support to combat veterans and MST survivors — with fewer enrollment requirements than VA medical centers.
- Veterans Crisis Line: 988, press 1 — available 24/7 for crisis support, referrals, and mental health resources.
- PTSD Coach app: A free mobile application developed by the VA National Center for PTSD, providing psychoeducation, symptom tracking, coping skills, and connection to professional care.
What Should You Do Next?
PTSD in veterans is a serious, life-threatening, and highly treatable medical condition. The 2023 VA/DoD Clinical Practice Guideline identifies multiple first-line psychotherapies — CPT, PE, and EMDR — with strong evidence bases demonstrating significant, durable symptom reduction. Intensive treatment formats with completion rates above 87% address the dropout problem that has historically limited outcomes in weekly-format care. The VA’s $17 billion mental health investment and expanded telehealth infrastructure are reducing access barriers that have long delayed treatment for veterans in underserved areas.
To connect with evidence-based PTSD care:
- Contact the VA National Center for PTSD (ptsd.va.gov) to find VA-affiliated PTSD clinicians, locate a Vet Center, or access self-help resources, including the PTSD Coach app.
- Call the Veterans Crisis Line at 988, then press 1, for immediate support. Text 838255 or chat at VeteransCrisisLine.net.
- Ask specifically for a trauma-focused therapy — CPT, Prolonged Exposure, or EMDR — when seeking a mental health referral. These are first-line, not last-resort treatments, and asking by name helps ensure appropriate care.
- Inquire about intensive outpatient formats if weekly appointment adherence has been a previous barrier — IOP completion rates are nearly double those of standard weekly care.
Talk to a licensed mental health provider or VA clinician who specializes in trauma-focused therapy for veterans to determine the type, format, and intensity of PTSD treatment that best matches your current needs and situation.
References
Biscoe, C., Lancaster, G., Jones, A., & Murphy, D. (2024). Complex PTSD symptom clusters and executive function in UK armed forces veterans: A cross-sectional study. BMC Psychology, 12(1), 87. https://doi.org/10.1186/s40359-024-01594-x
Forehand, J. A., Dufort, V., Gradus, J. L., Maguen, S., Watts, B. V., Jiang, T., Holder, N., & Shiner, B. (2022). Association of PTSD severity and death by suicide. British Journal of Psychiatry. https://doi.org/10.1192/bjp.2022.110
Holder, N., Shiner, B., Li, Y., & Lipschitz, J. (2024). Which veterans with PTSD are most likely to report being told of their diagnosis? Psychiatric Services, 75(1). https://doi.org/10.1176/appi.ps.20230101
Lang, A. J., Hamblen, J. L., Holtzheimer, P., Kelly, U., Norman, S. B., Riggs, D., Schnurr, P. P., & Wiechers, I. (2024). A clinician’s guide to the 2023 VA/DoD Clinical Practice Guideline for Management of Posttraumatic Stress Disorder and Acute Stress Disorder. Journal of Traumatic Stress, 37(1), 19–34. https://doi.org/10.1002/jts.23013
Leighton, S. C., Nieforth, L. O., & O’Haire, M. E. (2024). Assistance dogs for military veterans with PTSD: A systematic review, meta-analysis, and meta-synthesis. Clinical Psychology Review, 108, 102382. https://doi.org/10.1016/j.cpr.2024.102382
McLean, C. P., & Foa, E. B. (2024). State of the science: Prolonged Exposure therapy for the treatment of posttraumatic stress disorder. Journal of Traumatic Stress, 37(4), 535–550. https://doi.org/10.1002/jts.23046
Mission Roll Call. (2025). The state of veteran post-traumatic stress (2025 update). https://missionrollcall.org/veteran-voices/articles/the-state-of-veteran-post-traumatic-stress/
nchstats.com. (2025). Mental health trends among veterans: PTSD and suicide risk by state. https://nchstats.com/mental-health-among-veterans/
Ortiz Diaz, K. J., Landes, S. D., & Monnat, S. (2024). Differences in post-traumatic stress disorder (PTSD) between U.S. civilians and military veterans in the Gulf War and post-9/11 war eligibility cohorts: A research note. Armed Forces & Society. https://doi.org/10.1177/0095327X241233748
PTSD Research Quarterly (National Center for PTSD). (2024). Massed and brief treatments for PTSD. PTSD Research Quarterly, 35(3). https://www.ptsd.va.gov/publications/rq_docs/V35N3.pdf
RAND Corporation. (2025). The rising rate of suicide among veterans. RAND Perspectives, PEA1363-1-v2. https://www.rand.org/pubs/perspectives/PEA1363-1-v2.html
Schnurr, P. P., Hamblen, J. L., Wolf, J., Coller, R., Collie, C., Fuller, M. A., Holtzheimer, P. E., Kelly, U., Lang, A. J., McGraw, K., Morganstein, J. C., Norman, S. B., Papke, K., Petrakis, I., Riggs, D., Sall, J. A., Shiner, B., Wiechers, I., & Kelber, M. S. (2024). The management of posttraumatic stress disorder and acute stress disorder: Synopsis of the 2023 VA/DoD Clinical Practice Guideline. Annals of Internal Medicine. https://doi.org/10.7326/M23-2757
Stellman, J. M., Stellman, S. D., & Park, A. (2025). Impact of persistent combat-related PTSD on heart disease and chronic disease comorbidity in aging Vietnam veterans. Journal of Occupational and Environmental Medicine. https://doi.org/10.1097/JOM.0000000000003261
U.S. Department of Veterans Affairs. (2024). VA 2024 National Veteran Suicide Prevention Annual Report. https://news.va.gov/137221/va-2024-suicide-prevention-annual-report/
VA National Center for PTSD. (2025). Overview of psychotherapy for PTSD. https://www.ptsd.va.gov/professional/treat/txessentials/overview_therapy.asp
Share This Post

TREATMENTS WE OFFER
Are you covered for treatment?









LAOP is an approved provider for Blue Shield of California and Magellan, while also accepting many other major insurance carriers.
Check Coverage Now!

